





Abstract
Ectopic thyroid tissue, 90% presenting in lingual zone, is often scanned by ultra-sonography or computed tomography. Most surgeons regard ectopic thyroid as metastatic foci from thyroid cancer, thus resection is recommended. Here, we reported a man with bilateral papillary thyroid cancer, accompany with normal ectopic thyroid tissue in right sternocleidomastoid muscle. In this case, we highlighted: (i) It is rarely reported that ectopic normal thyroid tissue presented in sternocleidomastoid muscle. (ii) The ectopic thyroid tissue may not always be metastatic foci even though bilateral thyroid tumors were confirmed to be papillary cancer. (iii) Contrary to radical excision of all ectopic thyroid tissue, we advocate that only patients who need to receive the radioactive iodine therapy after total thyroidectomy should remove the ectopic normal thyroid tissue.
INTRODUCTION
Since the first document on ectopic thyroid in 1749, it has been subsequently reported. Lingual thyroid cases represent almost 90% of all ectopic thyroid cases, whereas lateral aberrant thyroid is much rarer described. Some researchers recommend treating ectopic thyroid as normal thyroid tissue, however, most surgeons advocate that we should remove it as metastatic foci from thyroid carcinoma. In this case, we reported a man affected with bilateral papillary thyroid cancer, accompany with right lateral aberrant normal thyroid tissue.
CASE REPORT
A 43-year-old man presented in 2021, with bilateral thyroid nodules detected by ultra-sonography 5 months earlier. He had no night sweats, no respiratory or dysphagia difficulty, nor other pressure symptoms. An ultrasound scan interpreted nodules in left and right thyroid gland, which were irregular defined, low-echo with calcification. In addition, there was a mass measured about 28 × 5 × 20 mm in front of internal jugular vein. Fine needle aspiration biopsy was advised and histological investigation showed bilateral papillary thyroid cancer. Therefore, total thyroidectomy was recommended.
The patient was hospitalized in 22 March 2021. The level of thyroglobulin was as high as 230.80 ng/ml, whereas all other thyroid functional indicators were normal. Chest and abdominal examination as well as preoperative fiberoptic laryngoscopy were all normal. He underwent contrast-enhanced cervical computed tomography (CT) scan, which confirmed bilateral possible malignant nodularity in thyroid gland and an ~1.6 × 0.6-cm hyperdensity deep to the right sternocleidomastoid muscle (SCM, Fig. 1A). Total thyroidectomy and bilateral central neck dissection was operated. A metastatic lymph node encapsulated the left recurrent laryngeal nerve. In the same time, the mass lateral to the right SCM was removed, which was separated from the thyroid gland (Fig. 1B). Intraoperative neuromonitoring information was normal. Pathology demonstrated bilateral papillary thyroid cancer (the size of cancer in left lobe was 2.2 cm, right 1.6 cm) with three lymph node metastases. However, the aberrant thyroid was histological free of cancer. Postoperative radioactive iodine therapy (RAI) was recommended for this patient.
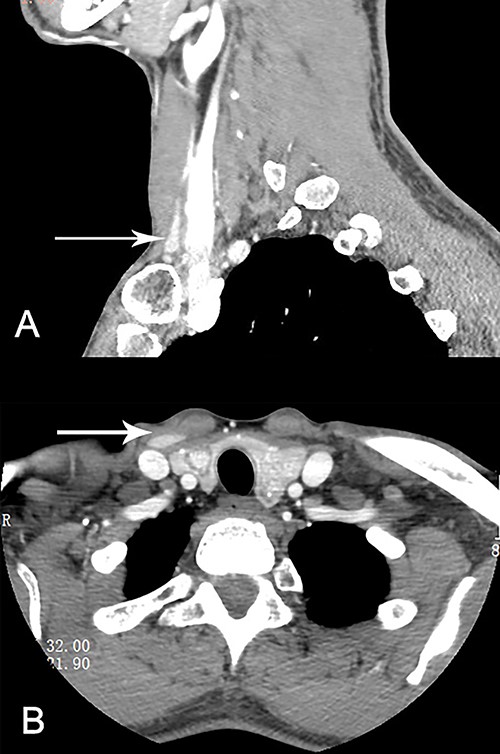
Ectopic lateral thyroid in CT (as is shown in white arrow in A and B).
DISCUSSION
Ectopic thyroid was described as thyroid tissue, which was located anywhere other than the pretracheal region, most frequently in the lingual position. Ectopic thyroid was mostly due to the aberrant migration and development of normal thyroid gland [1]. Chrispin argued that the migration of normal thyroid cells after operation may also contribute to the formation of ectopic thyroid [2]. King et al. suggested that ectopic thyroid tissue should be regarded as lymph node metastatic foci from papillary thyroid carcinoma [3]. Thus, in one time, it was recommended that ectopic thyroid tissue should be removed as metastatic foci from thyroid cancer. However, with the increasing number of relevant reports, more and more benign ectopic thyroid tissues were identified. Researchers revealed that > 70% ectopic thyroid was confirmed to be benign [4]. In some case, ectopic thyroid tissue may be the only thyroid tissue since the normal thyroid tissue was absent in 75% patients suffered with lingual thyroid [5]. Thus, unnecessary excision of ectopic thyroid may cause hypothyroidism. Yet, in cases like the present one, total thyroidectomy without excision of the lateral ectopic thyroid may attenuate the effect of RAI.
Considering relevant documents, we highlight that: if no detectable malignant tumor in ectopic thyroid tissue whose normal anatomy thyroid was absent, resection of ectopic thyroid should be circumspect. However, patients who need to receive the RAI therapy after total thyroidectomy should remove the ectopic thyroid tissue.
CONFLICT OF INTEREST STATEMENT
None delcared.
FUNDING
None.

{kind=link}