





Abstract
Although transurethral resection of the prostate is still standard of care in many patients suffering from benign prostatic hyperplasia, traditional open prostatectomy (OP) seems as a widely applied method in larger glands. In spite of the fact that holmium laser enucleation can be performed in large glands, upper limits of prostate size in this method are not clearly identified in the current literature. In this case, we aim to report feasibility and efficacy of OP in huge prostate size measured as 680 ml by transrectal ultrasound and review the current literature.
INTRODUCTION
Benign prostatic hyperplasia (BPH) is one of the most common diseases in middle age or older men [1]. This disease is determined by benign prostatic enlargement, which may cause lower urinary tract symptoms that include both obstructive and voiding symptoms. Diagnostic tools commonly include digital rectal examination (DRE), prostate volume evaluation, uroflowmetry, determination of International Prostate Symptom Score (IPSS), serum prostate-specific antigen level (PSA) and post-void residual urine (PVRU). Patients who suffered from BPH may be treated either medically or surgically. Although medically treatment is well established with alfa-1 adrenoreceptor antagonists and 5 alpha-reductase inhibitors, surgical procedures may be differ due to insufficient endourological equipments and resources, especially in the developing countries, and prostate size varying from patient to patient. In this study, we report an older man with huge prostate size that is measured 680 ml by transrectal ultrasound (TRUS) and treated with transvesical simple prostatectomy.
CASE REPORT
A 83-year-old male patient presented to our institution with a decrease in the caliber and force at the urinary stream. There were no relevant comorbidities such as diabetes mellitus, heart failure and neurologic disorders. Physical examination revealed that dullness to percussion on the suprapubic area suggested bladder distention. Consistency of prostatic parenchyma was benign and no suspicious nodule was handled at the dorsal surface of prostate in DRE. The serum PSA was 7.120 ng/ml. Comprehensive analysis of blood parameters was virtually normal, except serum creatinine level was 4.72 ng/ml. Pyuria was detected at urine analysis, but urine culture was sterile. Transabdominal ultrasound showed bilateral, severe hydronephrosis secondary to globe vesicale and prostate was measured as 680 ml by TRUS. Urethral catheterization was done and patient was observed at the clinic with proper fluid and drug therapy. First of all, patient received diagnostic cystoscopy in order to rule out concomitant malignancy, urethral stricture and determination of bilateral ureteral orifice location under general anesthesia. Subsequently, patient was placed in supine position. A vertical midline incision was made to reach Retzius space. Intravesical component of the prostate was identified and ureteral orifices were clearly located after vertical cystotomy. An incision in the posterior aspect of the prostate was made by electrocautery. The prostatic capsule was sharply freed from the adenoma with the surgeon's finger. After the adenoma completely freed from its attachments, prostate was removed from the surgical field. Homeostasis was achieved using a no. 1 polyglactin suture in a figure-of-eight fashion at 5:00, 7:00, 11:00 and 1:00 positions. A 22-French Foley catheter with a 40 ml balloon was placed transurethrally. The bladder was closed in two layers and Jackson-Pratt drain was also placed. No intra- or postoperative complication was noted. The removed specimen was 16 × 10 × 7 cm in size and weighed 540 g (Figure 1). A Foley catheter was removed and patient was discharged at postoperative day 5. Qmax and Qort values were recorded as 29 and 17 ml/s in uroflowmetry, respectively and patient did not suffer any complaints related to BPH at the postoperative 6th month.
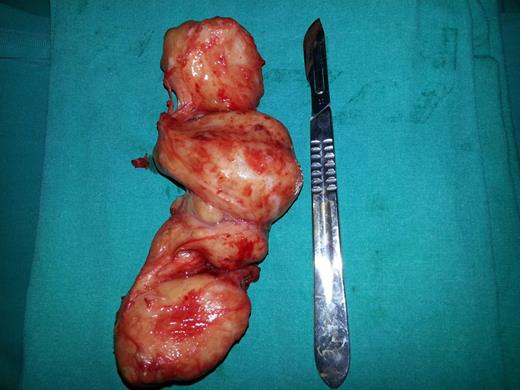
Final open prostatectomy specimen weighed as 540 g.
DISCUSSION
Transurethral resection of prostate (TUR-P) is still the gold standard procedure in the management of BPH [2]. In recent decades, together with technological advancement and advent of digital imaging, other minimally invasive surgical techniques such as laser treatments, transurethral incision of the prostate, transurethral microwave therapy and transurethral needle ablation of the prostate have also been performed in selected cases [3]. However, there is no enough evidence regarding the upper size limit of the prostate that amenable to TUR-P in the current literature. Additionally, TUR-P cannot be suitable in patients with a large median lobe due to completely obstructed trigone, invisible ureteral orifice and ultimately high recurrence risk. Any of the aforementioned minimally invasive techniques except holmium laser enucleation (HoLEP) and transurethral photoselective vaporization of the prostate (PVP) have not been achieved valid indication for large glands [4].
Two randomized controlled studies have shown that HoLEP has comparable outcomes with open surgery in terms of improving micturition and low re-operation rates [5, 6]. Furthermore, these studies declared that HoLEP was better than OP in terms of blood loss, catheterization and length of stay. However, HoLEP requires significant surgeon expertise and available surgical equipments. Therefore, traditional OP is still seen as the first-line treatment modality in men with prostate size of >80 ml, especially in developing countries. Published literatures have shown that OP improves IPSS points and Qmax values in the range of 62–86 and 86–677%, respectively. Changes in PVRU volumes have also been noted as 77–287 ml [5–7]. Moreover, Gratzke et al. have showed acceptable early postoperative results with expected complication rates. In this study, 902 patients who underwent OP were analyzed prospectively. Mean prostate size was 96.3 ml, and average enucleated tissue was noted as 84.8 g. Nevertheless, overall complication rate was 17.3%; statistically significant improvements were reported in terms of Qmax values and PVRUs. The authors finally concluded that OP had a still viable option for large glands with no requirement of modern minimally invasive methods such as HoLEP [8].
Though OP can be seen as a most invasive surgical approach in the management of BPH, it provides excellent symptomatic improvements and lowest failure rate even in men with significant benign prostatic enlargement and median lobe. This case report shows that OP can provide safe and effective improvement of symptoms even in patients with very large glands. In this case, we successfully treated severe infravesical obstruction due to giant prostate gland, which was measured as 680 ml, and grade 3 intravesical prostatic protrusion. No complication was recorded. Spontaneous regression of bilateral hydronephrosis was observed and patient was relieved of all his complaints secondary to intravesical obstruction at the last follow-up.
In conclusion, OP can be considered as the first-line treatment approach in the management of BPH with large prostate when the optional minimally invasive techniques such as HoLEP and PVP are not available. This procedure can be achieved more accurate and durable symptom relief even in glands weighing over than 600 ml.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}