





Abstract
Sliding hernias are those in which part of the sac wall is formed by a retroperitoneal organ and/or its mesentery protruding outside the abdominal wall cavity. The hernia sac may contain jejunum, ileum, vermiform appendix, Meckel's diverticulum, stomach, ovary, fallopian tube or urinary bladder. Our report features an adult case with cryptorchidism in which testis and spermatic cord constitute a component of the indirect inguinal hernia sac.
INTRODUCTION
Sliding hernias are those in which part of the sac wall is formed by a retroperitoneal organ and/or its mesentery protruding outside the abdominal wall cavity [1]. The hernia sac may contain structures such as cecum, ascending colon or appendix on the right side, the sigmoid colon on the left side or the uterus, fallopian tubes, ovaries, ureters and bladder on either side [2].
CASE REPORT
A 33-year-old male patient was admitted to the emergency clinic with complaints of abdominal pain accompanying a mass in the right inguinal region of >1 day's duration. A physical examination revealed an irreducible mass, thought to be an incarcerated inguinal hernia. Under spinal anesthesia, after dissecting the external oblique aponeurosis and opening the inguinal canal, a hernia sac was found that originated from the deep inguinal ring, extending along the canal and terminating just proximal to the external orifice. The spermatic cord could not be identified or separated from the hernia sac. A hard mass was palpated in the hernia sac, which suggested the presence of testis. We were unable to separate the testis from the wall of the sac (Fig. 1). After a urology consultation, it was decided to perform an orchiectomy due to the atrophic appearance of the testis and the relative risk of malignancy development. The testis and the spermatic cord were resected within the hernia sac by high ligation. A Lichtenstein tension-free herniorrhaphy was performed using propylene mesh. The patient's postoperative course was uneventful and he was discharged on the first postoperative day. Further histopathological examination of the hernia sac revealed a sliding hernia in which a part of the wall consisted of testis and ductus deference (Fig. 2).
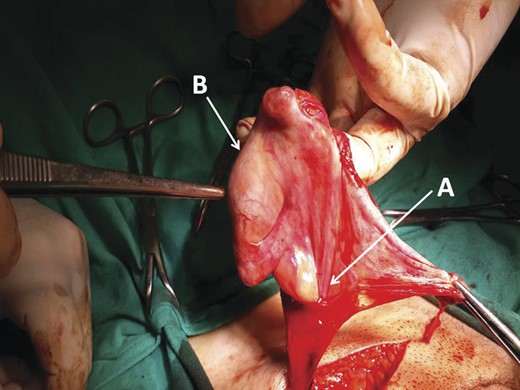
Sliding indirect inguinal hernia sac. (A) The hernia sac. (B) Testis constitutes a component of the hernia sac.
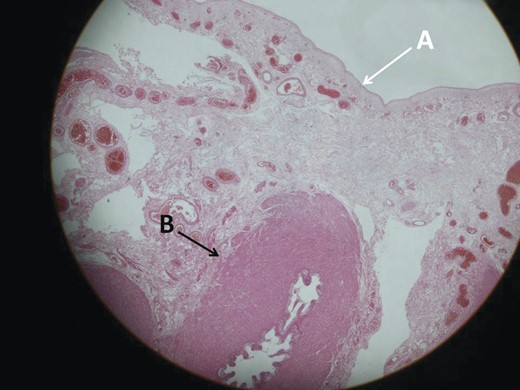
Microscopic section of the hernia sac. (A) Inside of the hernia sac. (B) The ductus deference makes up a part of the sac wall (H&E ×20).
DISCUSSION
During fetal development, testis descent from the abdominal cavity to the inguinal canal takes place between 8 and 15 gestational weeks. Insulin-like hormone 3 is the primary regulator of this phase, possibly augmented by Mullerian-inhibiting substance/anitmullerian hormone, and regression of the cranial suspensory ligament by testosterone. The testis may further descend through the inguinal canal to the scrotum at 25–35 weeks, which is controlled by androgens acting both directly on the gubernaculum and indirectly via the genitofemoral nerve, and release of calcitonin gene-related peptide from its sensory fibers [3]. Deflection in the regulatory mechanism may result in a variety of structural defects such as indirect inguinal hernia, hydrocele, undescended testis, interparietal hernia or Spigelian hernia [4]. There is one report of a male cryptorchid infant who had an interparietal hernia that contained testis in its wall. In this case, the hernia sac passed through the deep inguinal ring and extended superiorly to the anterior abdominal wall between the external oblique and internal oblique aponeurosis [5]. In contrast to this case, our patient had a well-developed inguinal canal with a rudimentary gubernaculum. Additionally, to our knowledge, our patient is the first reported case of an adult with a sliding indirect inguinal hernia where the hernia sac wall contained testis.
In conclusion, aberrations in the regulatory mechanism of hormones and peptides that have an effect on testicular descent may lead to a variety of structural anomalies such as incomplete or absence of the inguinal canal; absence or rudimentary developed gubernaculum; cryptorchidism; aberrant hernia localizations such as Spigelian hernias and sliding inguinal hernias that may contain tuba ovaries or testis. Future studies should be focused on these hormonal mechanisms to better understand and define the underlying physiopathology.
CONFLICT OF INTEREST
The authors declare that they have no conflict of interest.

{kind=link}
{kind=link}
{kind=link}
{kind=link}