





Abstract
Metastasis of any kind to the patella is rare. Metastasis to the patella causing symptoms representing the first presentation of underlying malignancy is rarer still. We report the case of a previously fit and well 74-year-old male presenting with left anterior knee pain. The initial diagnosis was osteoarthritis but after continued symptoms a diagnosis of solitary patella metastasis from a primary renal cell carcinoma was confirmed.
INTRODUCTION
Metastasis of any kind to the patella is rare and usually due to breast or lung malignancy [1]. Symptomatic metastasis to the patella representing the first presentation of an underlying malignancy is rarer still. To our knowledge this case represents the first documented report of a case of renal cell carcinoma (RCC) presenting with knee pain due to patella metastasis.
CASE REPORT
We present the case of a 74-year-old Caucasian male presenting with a 2-year history of left knee pain. He described difficulty kneeling and descending stairs. On examination, a tender and mildly diffuse swelling was present over the left patella associated with mild erythema. The patient was able to perform a straight leg raise test and had full range of movement of the left knee. Ligamentous and meniscal testing was unremarkable as was examination of the ipsilateral hip.
Nineteen months earlier the patient had consulted his general practitioner complaining of left knee pain. Radiographs performed at that time were reported to show joint space narrowing within the patello-femoral compartment as well as early joint space narrowing within the medial compartment. A subchondral lucency was also noted within the patella which was described as a subarticular cyst secondary to the previously mentioned patello-femoral degeneration (Figs 1–3).
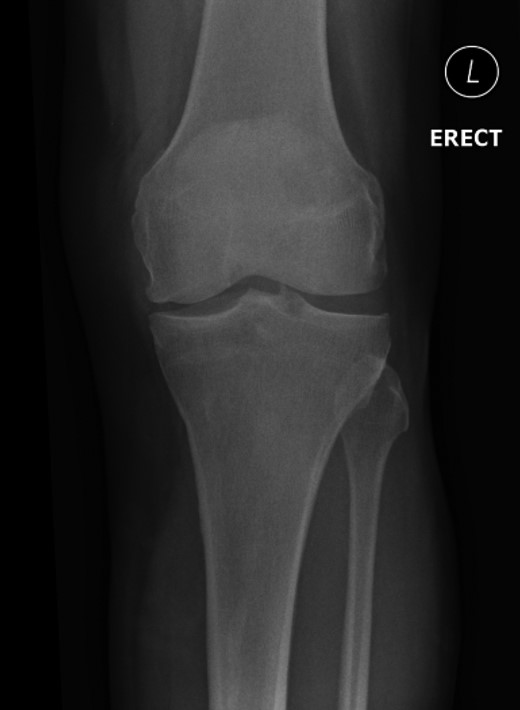
AP view: left patella at initial presentation.
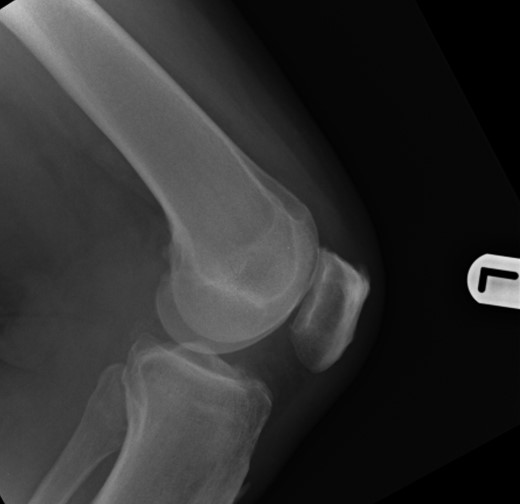
Lateral view: left patella at initial presentation.
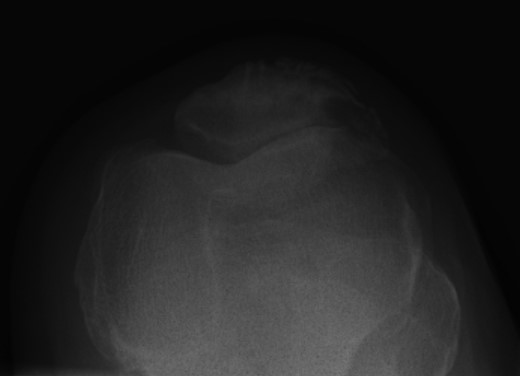
Skyline view: left patella at initial presentation.
The patient had a past history of prostate cancer, diagnosed in October 2005. He had been successfully treated and discharged from follow-up. In August 2007 he underwent excision of a basal cell carcinoma and had a permanent pacemaker for bradyarrhythmia. His only regular medication was a statin. Overall, he enjoyed good health and considered himself very active. There were no symptoms or signs of systemic disease.
Repeat radiographs performed by his general practitioner 19 months after initial presentation (Figs 4–6) revealed a large lucency within the patella and a discontinuity in the anterior cortex of the inferior pole suggesting pathological fracture. A bone scan was arranged and demonstrated isolated abnormal tracer activity around the left patella (Fig. 7). Due to the pacemaker a computed tomography (CT) scan was performed to further characterize the lesion. This confirmed a large lucent area occupying most of the patella with multiple areas of cortical disruption along its anterior border (Fig. 8). Since the exact nature of the lesion could not be determined an ultrasound-guided biopsy was suggested but ultrasound screening revealed the lesion to be highly vascular (Fig. 9). In view of this the radiologist performed a renal ultrasound, which revealed a large mass arising from the superior pole of the left kidney. Subsequent CT of the chest, abdomen and pelvis followed demonstrating the extent of disease. There was a large (13 × 8.5 × 9 cm) mass arising from the superior pole of the left kidney (Fig. 10), the appearances of which were consistent with a primary RCC. Metastases were found in both adrenals and lungs, but no other bone metastases. Since diagnosis, the patient has had a left nephrectomy and is currently receiving radiotherapy and zolendronic acid treatment for the patella metastasis. At the time of writing this report the patient's patella lesion continues to be managed non-operatively.

AP view left patella at subsequent presentation.

Lateral view: left patella at subsequent presentation.
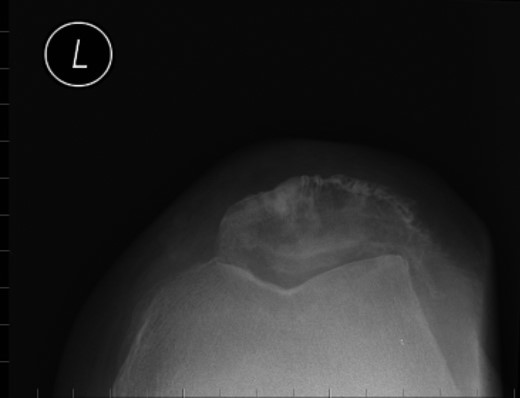
Skyline view: left patella at subsequent presentation.
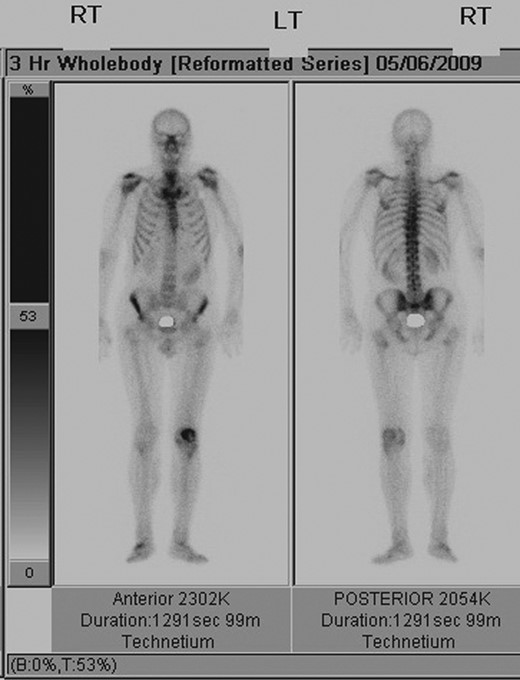
Whole-body bone scan demonstrating isolated increased tracer uptake around the left patella.
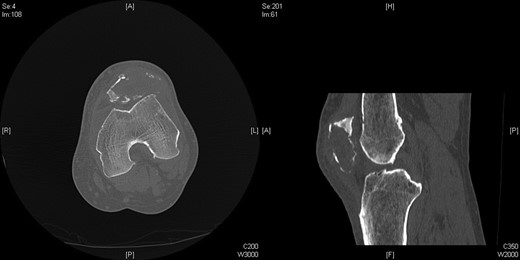
Axial and sagittal CT Images of left patella.
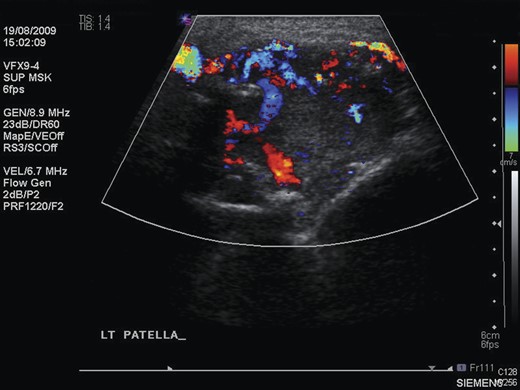
Ultrasound scan of the left patella, showing extensive neovascularization and increased flow within the lesion.
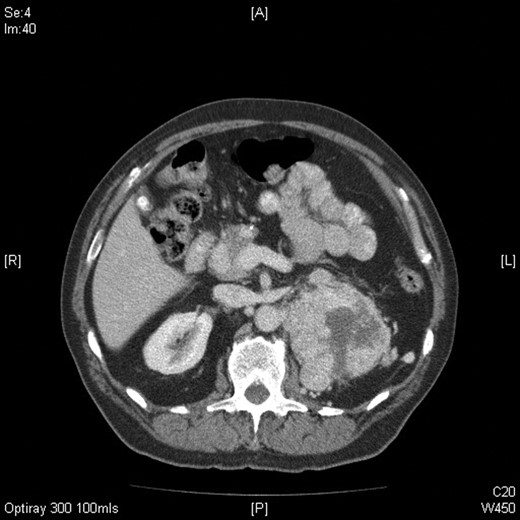
Axial CT image of the abdomen confirming the presence of a large mass arising from the superior pole of the left kidney measuring 13 (craniocaudal) × 8.5 (side to side) × 9 (AP) cm with central areas of necrosis.
DISCUSSION
Up to 30% of patients with RCC present with symptoms due to metastatic disease. The classic triad of haematuria, loin pain and loin mass is uncommon (10%) and is usually only seen in advanced cases [2].
Excluding leukaemias the most common form of bone neoplasm is metastatic carcinoma. The most frequent tumours to metastasise to bone in adults are carcinomas of the lung, prostate, breast, thyroid, kidney and colon. Tumours of the patella are extremely rare and account for <1% of primary bone tumours. Uniquely, primary tumours of the patella are more common than metastatic deposits and are usually benign with the most common being giant cell tumours [3].
This case represents only the fourth documented case, in English literature, of metastatic disease within the patella to originate from RCC [4–6] and the only such instance of anterior knee pain as the presenting complaint.
The absence of associated features of systemic disease, as well as radiographic appearances in keeping with early patello-femoral osteoarthritis (OA), account for the delay in diagnosis. The initial images suggest mild degeneration but, whilst subarticular cysts are a radiographic feature of OA, the lesion shown in this case is larger than would be expected with the level of disease shown elsewhere in the joint.
Unfortunately, knee pain is a hugely common complaint and it is therefore very easy to overlook diagnoses other than OA, particularly in older patients.
This case highlights a simple yet powerful learning point: potentially incongruous lucencies within bone mandate careful consideration of the differential diagnosis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}