





Abstract
Here we report an unusual case of small bowel obstruction, preluded by an unremarkable presentation of appendicitis. The small bowel obstruction subsequently diagnosed involved deposition of an appendicolith within the small bowel. Radiographic features of this incident are discussed along with its pathomechanics. Surgical management was carried out and is detailed along with advice for the management of retained appendicolith.
INTRODUCTION/BACKGROUND
Appendectomy is one of the most frequently performed general surgical procedures in the western world. Complications including re-operation and intra-abdominal sepsis and are markedly increased in those patients with perforation [1]. An appendicolith promotes appendicitis and increases the risk of appendiceal perforation. In a perforated appendix it can escape into the peritoneal cavity, before or during appendectomy. It is known to be associated with post-operative complications, predominantly in relation to abscess formation and intra-abdominal sepsis [1].
Here we present what we believe to be the first case of a mechanical small bowel obstruction secondary to a retained appendicolith, as an early complication of a conventional appendectomy for a perforated appendicitis.
CASE REPORT
An 18-year-old previously healthy female initially presented to the Emergency Department with a 2-day history of peri-umbilical pain which migrated to the right lower quadrant. On further questioning, she complained of anorexia and low grade fever. On examination, she had localized tenderness in the right lower quadrant with rebound tenderness over McBurney’s point. Her laboratory results revealed increased inflammatory markers, a normal urine dip and a negative pregnancy test. A clinical diagnosis of acute appendicitis was made, and she was taken to the operating theatre for an open appendectomy. The intraoperative findings confirmed a suppurating perforated appendix that was removed and sent for histology. In the first post-operative day, the patient was feeling very well with no further complaints, and a provisional plan for discharge was made (Figs 1–3).

Intraoperative picture showing retained appendicolith with adhered small bowel.

Intraoperative picture 2.
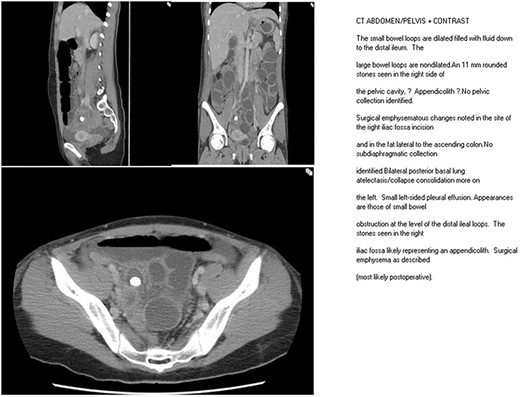
CT scan frame showing retained appendicolith.
Unfortunately, from Day 2, post operatively the patient started developing symptoms of nausea, vomiting and moderate abdominal pain. On examination, she had mild abdominal distension with minimal tenderness in the lower abdomen with no signs of peritonitis. Blood tests did not display any significant changes. The abdominal radiograph showed dilated small bowel loops and an appendicolith in the right iliac fossa. A computerized tomography scan was performed and demonstrated dilated small bowel loops down to the distal ileum and a 11 mm appendicolith/stone in the right side of the pelvic cavity with no pelvic collection or other positive findings. The clinical diagnosis was that of an ileus, and she was treated conservatively with analgesia, nasogastric intubation and intravenous fluids. In the next 24 hours, her symptoms did not resolve, the abdominal distension progressively worsened with increasing lower abdominal pain and peritonism.
Consequently, the clinical decision was to take the patient to the theatre for an exploratory laparotomy. At the time of exploration, there were grossly dilated small bowel loops up to a distance of 20–30 cm from the terminal ileum. At that transition point, there were small bowel loops adhered together causing a mechanical small bowel obstruction. In the centre of the adherent loops, an appendicolith was found that was indenting at the point of being cocooned within the wall of the small bowel and the mesentery. There was no perforation of the small bowel. The appendicolith was then retrieved and the loops of the small bowels released, followed by a thorough peritoneal lavage. After surgery, the patient had an otherwise uncomplicated recovery and was discharged on the third postoperative day.
DISCUSSION
Of the adult patients with appendicitis, 8–12% have radiographically visible appendicoliths, and as many as one third of the appendectomy specimens contain appendicoliths. The incidence of appendicoliths in children with acute appendicitis is even higher, affecting up to 50% of patients [2].
A retained appendicolith is a well-recognized condition after appendectomy in perforated appendicitis, and it is mainly complicated by intra-abdominal abscess formation and intra-abdominal sepsis [1]. Horst et al. [3] reported four retained appendicoliths in 554 patients undergoing appendectomy resulting in subsequent abscess formation from 14 days to 17 months following the appendectomy. Guillem et al. [4] reports a case of a dropped appendicolith post laparoscopic appendectomy that resulted in a recurrent pelvic abscess. Subhepatic [5] and subphrenic abscesses [6] have also been reported as late complications of retained appendicoliths. An ectopic appendicolith represents a rare cause of a tubo-ovarian abscess [7] and uncommonly is associated with fistulous tracts between the abdominal cavity and skin [8]. The retained appendicolith acts as a nidus for infection promoting abscess formation. In our case, the retained appendicolith was indented in the small bowel loops and, to our knowledge, uniquely caused mechanical small bowel obstruction with a mechanism that is not entirely clear.
Dropped or retained stones as well as clips from other intra-abdominal procedures have been associated with post-operative small bowel obstruction. Tekin et al. [9] report a case of mechanical small bowel obstruction secondary to spilled gallstones after laparoscopic cholecystectomy, and Kuehnel et al. [10] report a similar case due to retained loose linear cutter staples after laparoscopic appendectomy. It is possible that the appendicolith in this case report acted as an infected foreign body in the abdominal cavity comprising the centre of an acute inflammatory process. As a result, the surrounding small bowel loops adhered at that point in a concentric fashion around the appendicolith.
In conclusion, it is known that retained appendicoliths are strongly associated with intra-abdominal abscess formation as a late complication post-appendectomy. However, they can also induce a mechanical small bowel obstruction as an early event. It is therefore important to have a high suspicion of a retained appendicolith in every case of a perforated appendix. Pre-operatively, we advocate the use of abdominal radiographs and USS as an indicator of perforation as well as identifying the presence of a free appendicolith. Intra-operatively, appendicoliths identified should be removed to avoid the aforementioned complications. If an appendiceal perforation is identified, careful inspection of the abdomen and pelvis should be made to retrieve a possible floating appendicolith. In all cases of perforated appendicitis if no appendicolith is identified or if there is a case of a known dropped appendicolith during the procedure that is left in situ, not able to be retrieved, we suggest further imaging including computerized tomography and a percutaneous retrieval [1] to avoid any further complications.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}