





Abstract
Trigeminal schwannoma is the second most common schwannoma after vestibular schwannoma. Symptoms vary depending on the anatomical structures affected by the tumor, including facial pain, paresthesia, dizziness and ataxia. The primary goals are controlling the symptoms and the maintenance of cranial nerves’ integrity perioperatively. We report a 39-year-old lady who was complaining of mild right-sided headache, vision and hearing loss, right facial weakness and dysphagia. CT and MRI showed a large dumbbell-shaped tumor originating from the trigeminal fossa abutting the petrous and cavernous carotid artery and extending to the infratemporal fossa. An image-guided endonasal endoscopic removal was successfully done. Image-guided endonasal endoscopic removal of a trigeminal schwannoma abutting the petrous and cavernous carotid artery and extending to the infratemporal fossa is a safe, effective approach, as it offers excellent visualization, accurate localization and safe dissection of the tumor from the critical anatomical neurovascular structures surrounding it.
INTRODUCTION
Trigeminal schwannoma is a benign tumor originating from the sheath of any part the trigeminal nerve. They are the second commonest skull base schwannomas, after vestibular schwannoma, accounting for about 8% of all intracranial schwannomas [1]. Management of a trigeminal schwannoma extending to the infratemporal fossa is difficult owing to its proximity to the internal carotid artery and cranial nerves III–VI [2]. However, surgical excision is the definitive cure. Therefore, anatomical knowledge is crucial as well as selecting the best surgical approach [3]. Image-guided endonasal endoscopic surgery is considered the preferred strategy because it is minimally invasive and provides effective results [4]. Possible complications include cosmetic problems, facial nerve palsy, hearing loss, dental malocclusion and lacrimal dysfunction. However, the advantages of this approach outweigh the disadvantages as it allows a better visualization of the tumor and the adjacent structures, easy manipulation of vessels and nerves as well as decreased tissue damage [5].
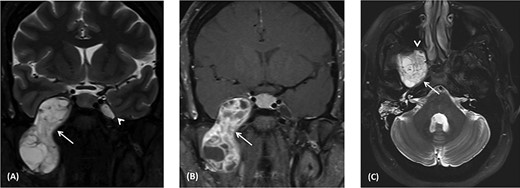
(A) Coronal T2 MRI shows dumbbell-shaped soft tissue mass with heterogenous high signal intensity across the widened oval foramen extending from the infratemporal fossa into Meckel’s cave (arrow). It displaces the temporal lobe superiorly and laterally. The left Meckel’s cave (arrowhead) is normal. (B) Coronal post-contrast T1 MRI shows heterogeneous enhancement of the right dumbbell mass across the right oval foramen (arrowhead). It shows multiple necrotic foci. (C) Axial T2 MRI shows heterogeneous high signal intensity mass at the level of foramen ovale abutting the petrous segment of the right internal carotid artery with no invasion (arrow). Anteriorly, the mass indents the posterior wall of the right maxillary antrum (arrowhead). Right mastoid air cells opacification secondary to obstructed right Eustachian tube.
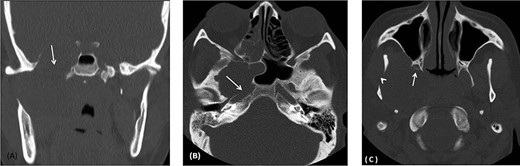
(A) Coronal CT image using bone window shows remodeling and widening of the oval foramen (arrow) secondary to infratemporal/middle cranial fossa mass. (B) axial CT images using bone window at the level of oval window demonstrates the widening of the canal with extension medially resulting in dehiscence of the anterior wall of the carotid canal (arrow). (C) Axial CT image using bone window at the infratemporal fossa level shows erosion and remodeling of the right pterygoid plates (Arrow) as well as the right mandible (arrowhead).
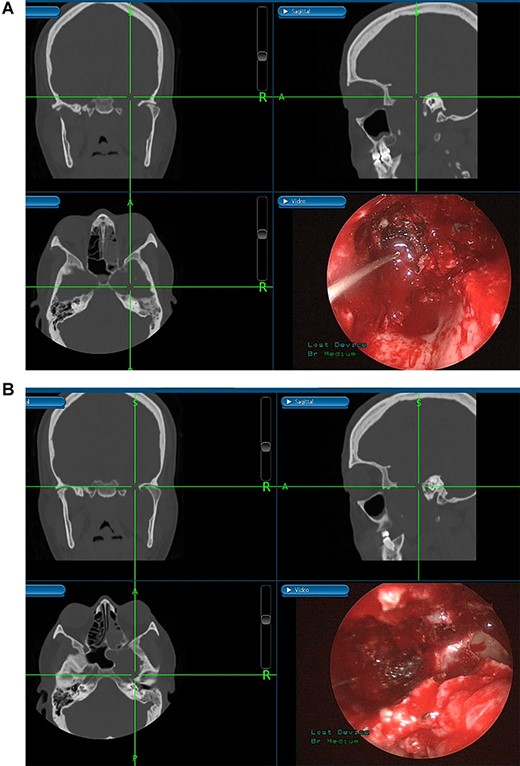
(A) Image-guided tumor removal from petrous carotid artery. (B) Image-guided intraoperative picture status post-complete tumor removal from trigeminal and middle cranial fossa.
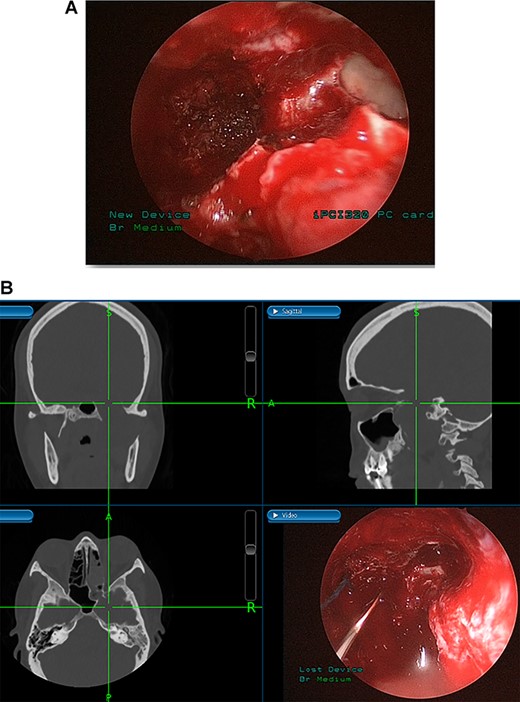
(A) Endoscopic view of the final surgical cavity after tumor removal. (B) Image-guided tumor removal from cavernous carotid artery.
CASE REPORT
A 39-year-old, medically free lady, was referred to our institute complaining of right-sided mild headache, vision and hearing loss, right facial weakness and dysphagia, for 3 months.
A magnetic resonance imaging (MRI) scan revealed a large dumbbell-shaped mass extending across the right skull base with intracranial and infratemporal fossa components in the path of the trigeminal nerve (Fig. 1A). It extends intracranially into the anteromedial aspect of the middle fossa into right Meckel’s cave with compression of the adjacent right cavernous sinus. The adjacent temporal lobe shows displacement laterally but no infiltration. Post-contrast images show heterogenous enhancement with solid and necrotic components (Fig. 1B). The posterior aspect of the skull base component of the mass abuts the horizontal segment of the right internal carotid artery along the carotid canal but without invasion (Fig. 1C). It compresses the right Eustachian tube with resultant opacification of the right mastoid air cells. The anterior aspect of the mass abuts the posterior wall of the right maxillary antrum. The overall appearance is likely representing schwannoma of the mandibular branch of the right trigeminal nerve.
Computed tomography (CT) scan shows remodeling and widening of the right foramen ovale (Fig. 2A). This is associated with focal dehiscence at the right lateral wall of the sphenoid sinus and the anterior wall of the right carotid canal (Fig. 2B). The lesion extends downwards to the infratemporal fossa with remodeling of the pterygoid plates (Fig. 2C) and the right mandibular ramus.
The patient underwent an image-guided endonasal endoscopic tumor removal starting by endoscopic medial and posterior walls maxillectomies to control the tumor removal from the lateral sphenoid sinus and the infratemporal fossa after cauterization of the maxillary artery and sphenopalatine artery branches feeding the tumor. The tumor was dissected and removed from the cavernous (Fig. 3A) and petrous carotid artery in the middle cranial fossa (Fig. 3B). The middle cranial fossa’s dura was intact during the tumor removal (Fig. 3C). All the steps of tumor removal were controlled and monitored under image-guided navigation for accurate localization of tumor removal and avoidance of violation to the middle cranial fossa’s dura, or the brain, and the internal carotid artery in its cavernous and petrous segments (Fig. 4a and b).
The final histopathological diagnosis showed low-grade mesenchymal neoplasm with degenerative changes consistent with trigeminal schwannoma.
The recovery and post-operative course was uneventful. The patient is keeping with good quality of life for 3 years post-treatment.
DISCUSSION
Trigeminal schwannoma is a mostly benign, solitary, slow growing tumor arising from Schwann cells of the myelin sheath, accounting for 1–8% of intracranial schwannomas and 0.1–0.5% of intracranial tumors [1]. Most common symptoms include facial pain and paresthesia, dizziness and ataxia. The infratemporal fossa is among the most challenging anatomical locations to access because of the adjacent vital structure [2]. Therefore, a thorough of the area’s anatomy is important to minimize the morbidity and chances of inadvertent damage. CT scan is always performed initially and may show widening of superior orbital fissure, foramen ovale or foramen rotundum, and also it depicts any erosions of the middle fossa and petrous apex. MRI is used to indicate the type of trigeminal schwannoma, adjacent anatomical structures and tumor volume [6]. Via imaging, the tumors are classified into six different types [7].
Anatomically speaking, infratemporal fossa contains vital neurovascular structures such as V3 and the internal maxillary artery. Inferiorly, it is occupied by the medial pterygoid muscle and the carotid artery posteriomedilay. The internal jugular vein and the cranial nerves IX–XII are in the post-styloid part of the parapharyngeal space. Furthermore, it includes other structures such as the pterygoid venous plexus, maxillary vein and the branches of the mandibular vein and chorda tympani nerves. The infratemporal fossa communicates with the pterygopalatine fossa medially via the pterygomaxillary fissure [8, 9].
Both open and endoscopic techniques are used to resect trigeminal schwannomas; they involve different steps and provide different degrees of exposure. The choice of modality depends mainly on tumor-nerve anatomical situation. The former approach is more suitable for tumors that locate trigeminal nerve medially while the latter is more suitable for tumors that locate it laterally [6].
Tumors in the infratemporal fossa require extensive approach such as middle fossa extraduaral approach, infratemporal fossa extradural approach, transmaxillary approach, transmandibular approach or transcervical approach. Complications from these procedures include cosmetic problems, facial nerve dysfunction, hearing loss and dental malocclusion. Image-guided endoscopic surgery allows for the preservation of intracranial structures, internal carotid artery and cranial nerves. Moreover, this procedure aids in rapid localization of the anatomical structures and meticulous intervention restricted to tumor margins. The screen is divided into four sections allowing visualization of the tumor from axial, coronal and sagittal views [10].
CONCLUSION
Image-guided endonasal endoscopic approach for Meckel’s cave trigeminal schwannoma abutting the petrous and cavernous carotid artery and extending to the infratemporal fossa is a safe and effective procedure. Advantages of this approach are excellent visualization, accurate localization and safe dissection and removal of the tumor from the critical anatomical neurovascular structures surrounding it.
ACKNOWLEDGEMENT
The authors declare that funding was not received from any party in order to conduct this study.
Conflict of interest statement. The authors certify that they have no affiliations with any organization or entity with any financial or other interests in the subject matter or materials discussed in this manuscript.

{kind=link}
{kind=link}
{kind=link}
{kind=link}