





Abstract
Small intestinal volvulus is rare in adults and rarely caused by string adhesions between the liver and the diaphragm. Similar adhesions were described in Fitz-Hugh-Curtis syndrome. We report a 45-year-old lady with small intestinal volvulus from entrapment of a loop in string adhesions between the liver and the diaphragm. Her plain radiographs showed a significant shadow of the trapped loop.
INTRODUCTION
Small intestinal volvulus rarely presents in adults. Violin string adhesions between the liver and the diaphragm seen in Fitz-Hugh-Curtis syndrome have been reported to cause large intestinal volvulus but not small intestinal volvulus. We report a 45-year-old lady with small intestinal volvulus from entrapment of a loop of ileum in string adhesions between the liver and the diaphragm. She presented with a significant shadow of the trapped loop on plain radiographs.
CASE REPORT
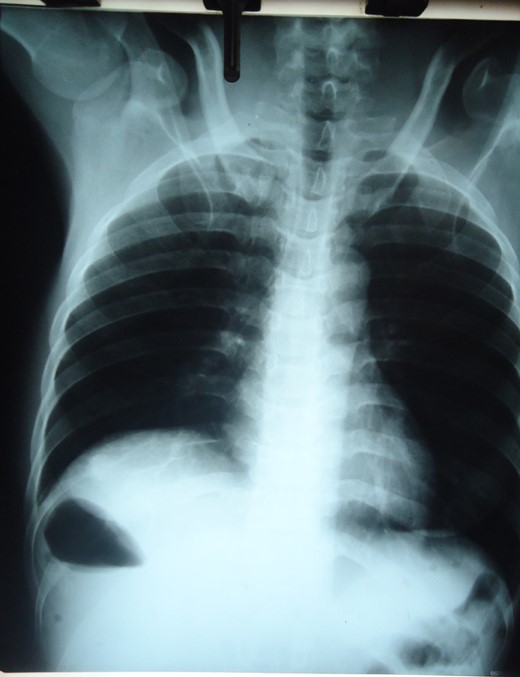
Chest X-ray showing right sub-diaphragmatic shadow with air fluid levels from trapped bowel.

Plain abdominal X-ray showing distended small bowel loops and right sub-diaphragmatic shadow with air fluid levels from trapped bowel.
Emergency laparotomy after resuscitation revealed that a loop of distal ileum trapped in string adhesions between the right lobe of the liver and the diaphragm was responsible for the right sub-diaphragmatic shadow with air fluid levels seen on the plain radiographs. The loop twisted around its mesentery and a segment of ~25 cm length was gangrenous. The loop passed anterior to the transverse colon and there was no defect in the mesentery. There were multiple whitish thin string adhesions between the diaphragmatic surface of the liver, the diaphragm and the anterior abdominal wall. The proximal small bowel was distended; the cecum was collapsed and edematous but viable. No other intra-peritoneal abnormality was found. A limited right hemi-colectomy and primary anastomosis was done and accessible string adhesions snipped. Post-operatively, she had anastomotic dehiscence that was managed with an ileostomy and she was discharged 49 days after surgery. She later had an Ileostomy take down and repair of incisional hernia. She has been followed for 3 years and has remained well.
DISCUSSION
Volvulus describes the rotation of a part or whole of the intestine along the axis of its mesentery. It leads to intestinal obstruction that may progress to gangrene. Small intestinal volvulus is rare in adults. It is seen more in some parts of Africa and Asia (24–60/100 000 population) than in western countries (1.7–5.7/100 000 population) [1]. Primary small intestinal volvulus occurs in an otherwise anatomically normal abdominal cavity with some attributed to bulky food intake during the fasting period [2]. Secondary small intestinal volvulus is associated with intra-operative findings of intra-abdominal abnormalities. Usually, the intestine twists along an abnormal point of fixation [3]. Congenital causes are more common in children and young adults and include internal hernias into peritoneal and mesenteric defects: Meckel's diverticulum, congenital bands and malrotations. Acquired abnormalities are most common in the sixth, seventh and eight decades of life and are commonly due to post-operative adhesions [4]. Other causes include pregnancy, ovarian cysts and tumors or cysts of the mesentery. Volvulus from post-operative internal hernias created after roux en Y anastomosis in liver transplantation and gastric surgery for morbid obesity and after ileostomy or bilroth II surgery are becoming more frequently seen. Hepato-diaphragmatic adhesions may not have been reported to cause small intestinal volvulus.
Violin string adhesion between the liver, the diaphragm and the anterior abdominal wall may follow perihepatitis that complicates pelvic inflammatory disease in Fitz-Hugh-Curtis syndrome [5]. Few cases have been reported in males [6]. Adhesions are usually asymptomatic and are incidental findings at laparotomy and laparoscopy. There are reports of association with large intestinal obstruction and volvulus, and a report with closed loop small intestinal obstruction. Volvulus from entrapment of the small bowel in string adhesions between the liver and the diaphragm is particularly interesting because the small intestine resides in the infra-colic compartment.
Small intestinal volvulus presents with severe colicky abdominal pains and vomiting that is difficult to differentiate from non-strangulating causes of intestinal obstruction. Early diagnosis and operative intervention is important to prevent gangrene seen in more than 40% of cases [3]. Mortality rates of 5.8–8% increases to 20–100% with gangrene [7]. Abdominal CT especially Multidetector CT with angiography is the most specific investigation [8]. Doppler ultrasonography showing the whirlpool sign is useful but operator dependent [9]. Plain radiography is insensitive in most cases. The plain radiographs of our patient showed a significant gas shadow below the right hemi-diaphragm that was discovered to be from entrapped bowel between the liver and diaphragm. An abdominal CT though more specific was omitted to minimize delay in the management. Radiological sign of hepato-diaphragmatic interposition of bowel loops was first described by Demitrus Chilaiditi in 1910 but the appearance in this patient differs from previous descriptions. Cases of Chilaiditi's syndrome have been reported in association with Fitz-Hugh-Curtis syndrome in large intestinal obstruction but none with small intestinal volvulus [10]. Treatment of small intestinal volvulus is derotation of the affected loop when viable and resection of gangrenous segments. Associated anatomical abnormalities are corrected by closure of intra-peritoneal defects, adhesiolysis or excision of mass lesions.
In conclusion, we report hepato-diaphragmatic adhesions as a cause of small intestinal volvulus in a lady with a significant radiological finding of sub-diaphragmatic gas shadows with air fluid levels. This finding may prove useful in management of similar presentation.

{kind=link}