





Abstract
Steal syndrome is characterized by the disruption of blood flow from specific vascular territories due to perfusion via collateral vessels bypassing an obstructed artery segment. In the neurovascular setting, this can lead to entities such as subclavian steal syndrome or the less prevalent double steal phenomenon, primarily associated with atherosclerosis. We present a case of an early 80s patient with cerebrovascular insufficiency who exhibited neurological deficits during mastication. The angiographic evaluation showed occlusion at the origins of the left common carotid and of the brachiocephalic trunk. This configuration caused the left vertebral artery to be the only vessel filling anterograde. The flow in the right vertebral artery is retrograde, filling the subclavian and the right common carotid artery. Endovascular revascularization of the brachiocephalic trunk was successfully performed using a Gore Viabahn VBX Balloon Expandable Stent (W.L. Gore & Associates, Flagstaff, AZ, USA), leading to symptom resolution.
Introduction
Steal syndrome arises when the distal segment of an obstructed artery receives perfusion through collateral vessels, thus diverting blood flow from neighboring territories. This phenomenon relies upon the vascular configuration, coupled with factors that may increase the demand for blood supply, potentially precipitating the apparition of clinical symptoms [1].
In the neurovascular setting, regarding the obstruction’s location and extent, patients could develop entities such as subclavian steal syndrome or the double steal phenomenon that could disrupt blood flow dynamics [2]. Such conditions have atherosclerosis as the main culprit, and it may lead to neurological claudication when there is an increase in flow demand. In stroke patients, the overall incidence of subclavian steal syndrome is 2.2% [3]; nonetheless, the incidence of the double steal phenomenon is even rarer, with scarce literature reports.
In extreme conditions, some patients only have one vessel supplying the brain. We present a case where a patient presented with cerebrovascular insufficiency partially compensated, manifesting syncopal and near syncopal episodes associated with an augmented hemodynamic requisition during mastication. This phenomenon is attributable to a superimposed left subclavian steal syndrome and occlusion of the brachycephalic artery, leading to a double steal phenomenon on the right.
Clinical presentation
A patient in their 80s was referred for neurovascular assessment due to syncopal episodes occurring during mealtime associated with mastication, the symptomatology was not present while eating soup or drinking liquids. The patient had a medical history of hypertension and underwent chemoradiation in 1999 for neck squamous cell carcinoma.
Postural changes and chewing led to recurrent transient loss of conscience causing the patient to lose weight due to a reduced solid food intake. She had no focal deficit during those episodes and her MRI did not reveal the presence of stroke.
A cerebral angiogram demonstrated left common carotid occlusion (Fig. 1A) and the occlusion of the origin of the right brachycephalic trunk (Fig. 1B). Consequently, the left vertebral artery is the only cerebral vessel from the aortic arch filling anterogradely, resulting in retrograde flow to the brachycephalic trunk and of the right common carotid artery and right vertebral artery (Fig. 2A–D). The left internal carotid artery is filled from the left occipital artery, which is filled by the left vertebral artery. Intracranially the patient has the posterior communicating artery and the anterior communicating artery.
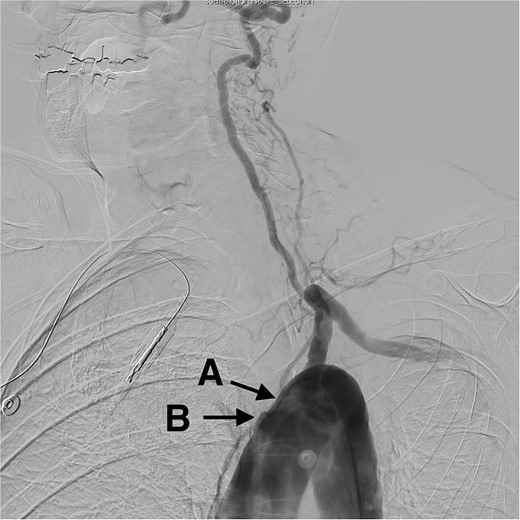
Digital subtraction angiogram demonstrating: (A) occlusion in the origin of the left common carotid artery. (B) Occlusion at the origin of the brachycephalic trunk artery.
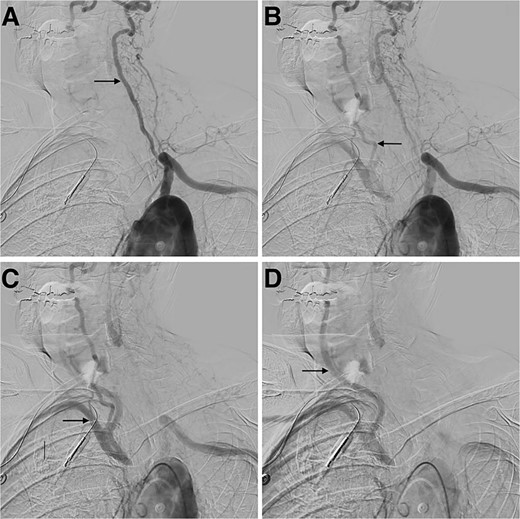
Digital subtraction angiogram demonstrating: (A) anterograde flow in the left vertebral artery and contrast going through the basilar formation. (B) Retrograde flow in the right vertebral artery. (C) Contrast reaching the right subclavian artery. (D) Anterograde flow in the right common carotid artery.
The patient was assessed for endovascular revascularization of the innominate artery. Right radial access and right femoral access were obtained. A pigtail catheter was advanced by the femoral access to obtain an aortic arch image and confirm the location of the catheter at the brachycephalic artery (Fig. 3A). Moreover, the radial access advanced a stiff glide wire, and a large bore catheter was advanced over it. Furthermore, a Gore Viabahn VBX Balloon Expandable Stent (W.L. Gore & Associates, Flagstaff, AZ, USA) was introduced and, under roadmap guidance, crossed the site of obstruction, completing the revascularization (Fig. 3B). The patient was discharged and referred for rehabilitation a few days later with a disappearance of the symptoms.
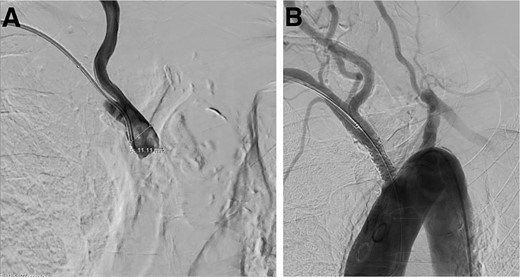
Digital subtraction angiogram demonstrating: (A) brachiocephalic artery occluded before the stent placement. (B) Brachiocephalic artery opened after the introduction of the Gore Viabahn VBX Balloon Expandable Stent (W.L. Gore & Associates, Flagstaff, AZ, USA).
Discussion
We presented a case of repeated transient loss of consciousness from cerebrovascular insufficiency in the context of innominate and left common carotid artery occlusion. Due to this configuration, the left vertebral artery is responsible for the entire brain’s blood supply. The left vertebral artery filled the basilar artery anterogradely. Retrogradely, through the right vertebral artery, it fills the right subclavian artery and, consequently, the right common carotid artery, resulting in the double steal phenomenon (Fig. 4) [4].
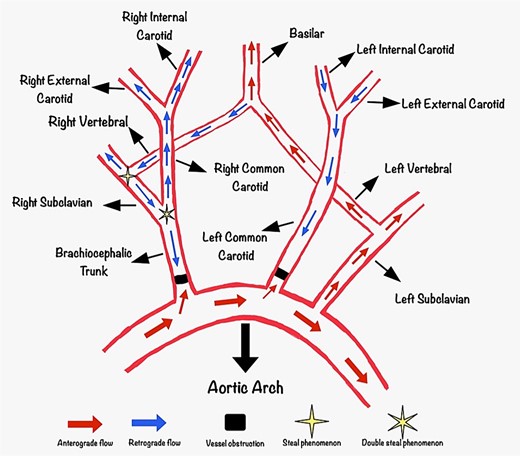
Diagram demonstrating the blood flow of the patient. Anterogradely the left vertebral artery fills the basilar artery and retrogradely fills the right subclavian artery and the common carotid artery through the right vertebral artery, resulting in a double steal phenomenon. The left internal carotid artery is filling from the left occipital artery in a retrograde flow fashion.
The therapeutic options which include stenting, bypass, or endarterectomy were discussed. Among these approaches, stenting was recommended and has now become the standard of treatment [2].
The episodes of syncope and near-syncope presented by the patient during the meals are explained by the fact that when there is mastication, supplementary blood flow from the left vertebral artery, which in this case supplies the entire cephalic circulation, is targeted to the masticatory muscles, decreasing the flow for the intracranial circulation. That mechanism is different from the cases where syncope is triggered by swallowing, a condition known as deglutition syncope [5]. Which is defined as lightheadedness or loss of consciousness during swallowing, and it is often associated with esophageal disorders and aberrant vagotonic reflex [6].
Conclusion
The coexistence of superimposed subclavian, double steal phenomenon, and extensive vessel occlusion can lead to an atypical clinical presentation. A strategic intervention achieved successful resolution of symptoms and allowed the patient to feed normally.
Author contributions
All the authors have contributed to this paper.
Conflict of interest statement
None declared.
Funding
None declared.
Patient consent
The patient consented to the procedure, and all identifiable information was removed from the images.
References
Author notes
Otavio F. De Toledo and Salvador F. Gutierrez-Aguirre contributed equally to this work and are joint first authors.

{kind=link}
{kind=link}
{kind=link}
{kind=link}