





Abstract
Interparietal hernias are rare and occur most commonly in the long-term postoperative setting following abdominopelvic surgery. This case report describes the development of a strangulated interparietal hernia through a defect in the posterior rectus sheath 4 days post-lower segment caesarean section (LSCS) in a 36-year-old female. Whilst she had an acute abdomen, she did not have a palpable incisional hernia. Her interparietal hernia was identified via a computed tomography scan of her abdomen and pelvis. She underwent a midline laparotomy where ischaemic small bowel was found within her hernia. This was resected and she had an unremarkable recovery. This case is the first of its kind and highlights the diagnostic challenge of interparietal hernias in acute postoperative patients as well as the importance of having a low threshold for suspicion for complicated interparietal hernias in patients with an acute abdomen following LSCS.
INTRODUCTION
We present the first case of a strangulated interparietal hernia 4 days following lower segment caesarean section (LSCS) resulting in the resection of 40 cm of distal ileum. Here we summarise the current literature and demonstrate the diagnostic dilemma of interparietal hernias. We also highlight the importance of having a low threshold for suspicion of interparietal hernias in any patient with an acute abdomen following LSCS.
CASE REPORT
Ms KF is a 36-year-old female who underwent an elective LSCS for a term delivery of one male infant. Following the caesarean, her peritoneum was closed with 2/0 vicryl and rectus sheath closed with 1 vicryl. During her pregnancy, she was taking clexane because of a history of venous thromboembolism (2014) in the context of Factor V Leiden and had gestational diabetes.
She had ongoing abdominal pain following her LSCS, which became severe on day 4 with associated bilious vomiting. The general surgical team was consulted. On examination, she was haemodynamically stable and afebrile, was writhing in the bed in pain and was firmer in her left and right lower quadrants with marked tenderness in comparison to upper quadrants on abdominal examination. Her serology was unremarkable. An urgent computed tomography (CT) abdomen pelvis demonstrated a 25 mm transverse defect in her posterior rectus sheath containing multiple loops of small bowel with submucosal and mesenteric oedema and free fluid within the hernial sac. The appearance was in keeping with a strangulated interparietal hernia containing small bowel (Fig. 1).
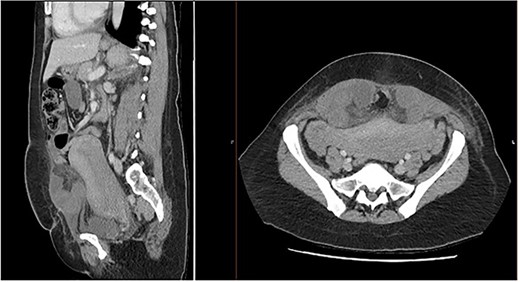
Sagittal and axial CT abdomen and pelvis slices demonstrating oedematous small bowel loops herniating between layers of the anterior abdominal wall.
A nasogastric tube (NGT) and indwelling catheter (IDC) were inserted, and she was taken emergently to theatres. Upon opening her Pfannenstiel incision, ischaemic small bowel was visualised through a defect in her anterior abdominal wall 10 cm superior to her Pfannenstiel incision necessitating a midline laparotomy. On further exploration, it was discovered that the posterior sheath at the level of the umbilicus was not closed allowing small bowel to herniate through and strangulate at this point (Fig. 2). A total of 40 cm of ischaemic ileum was divided with a gastrointestinal anastomosis (GIA) 80 and a side-to-side anastomosis with a GIA 80 and 3-0 vicryl to a common enterotomy was performed. Following copious washout with normal saline, clindamycin and gentamycin, a 24Fr Blake drain was inserted into her pelvis. Continuous one polydioxanone sutures were used to close peritoneum, fascia and her Pfannenstiel incision and continuous 0 vicryl sutures and staples were used to close her subcutaneous fat layer and skin, respectively.

Midline laparotomy demonstrating ischaemic ileum.
Postoperatively, her recovery was unremarkable. Her IDC and intravenous ceftriaxone and metronidazole were ceased 4 days following laparotomy and her NGT and pelvic drain were removed on Day 5. She was discharged home on Day 6 after having opened her bowels and tolerated a light diet. On follow-up, she has no evidence of any incisional hernias.
DISCUSSION
Originally described by Bartholin in 1661, interparietal hernias are defined as the protrusion of intraabdominal contents between layers of the anterior abdominal wall [1]. They occur rarely with a reported incidence of 0.01–1.6%. Lower and Hicken [2] in their 1931 case series of 587 interparietal hernias, additionally described three anatomical variants: preperitoneal (between the preperitoneum and transversalis fascia), interstitial (between the muscular layers of the abdominal wall) and superficial (between the external oblique muscle and skin). Whilst preperitoneal and superficial subtypes each accounted for 20% of the interparietal hernias in Lower and Hicken’s case series, interstitial were the most common comprising 60% [2]. Ms KF had an interstitial interparietal hernia.
Although posterior rectus sheath and interstitial interparietal hernias are discussed as separate entities in previous case reports, their definitions are the same and these terms can be used interchangeably. Posterior rectus sheath hernias can either be spontaneous/congenital, traumatic or post-surgical [3]. Even though the posterior rectus sheath is weakest below the arcuate line as it is only comprised of transversalis fascia, most spontaneous/congenital hernias occur superior to the arcuate line. Thus, it is hypothesised that the entrance of neurovascular structures into the posterior rectus sheath as well as predisposing factors such as those that raise intraabdominal pressure (such as pregnancy in Ms KF’s case) plays a role in the pathophysiology of posterior rectus sheath hernias [4].
Approximately 13 case reports on posterior rectus sheath hernias exist in the current literature with most cases developing in the long-term postoperative period (following previous robotic/abdominal hysterectomy, incisional/inguinal hernia repair, midline laparotomy) [3, 5–8]. However, to date, there have been no case reports on the acute development of a posterior rectus sheath hernia following LSCS. Interestingly, Ms KF’s defect was 10 cm superior to her Pfannenstiel incision. Thus, we hypothesise that this defect was created during the blunt longitudinal dissection of her fascia during entry and that a combination of the laxity of her fascia and the fascial closure technique (interrupted) contributed to the development of her hernia.
The diagnosis of a posterior rectus sheath hernia is challenging as it is often not visible or palpable because of the overlying abdominal wall musculature [3, 9]. This is even harder in acute postoperative patients who have had abdominopelvic surgery where it is difficult to distinguish hernia pain from regular postoperative pain and easy to assume that abdominal distension is rather secondary to either gas insufflation (if post-laparoscopy), a postoperative ileus or, in Ms KF’s case, her post-partum state. Whilst previous case reports have described the use of ultrasound and magnetic resonance imaging to diagnose posterior rectus sheath hernias, CT remains the imaging modality of choice as it can identify complications inside the hernia sac such as obstruction and strangulation [10].
In select cases of posterior rectus sheath hernias with symptoms of bowel obstruction, a diagnostic laparoscopy may be indicated [9]. However, the extent of lateralisation of Ms KF’s hernia sac (containing bowel) precluded safe port placement for a diagnostic laparoscopy. Thus, the decision was made to reopen her Pfannenstiel incision to explore her surgical wound. As with all other case reports of posterior rectus sheath hernias containing non-viable ischaemic bowel, a midline laparotomy and small bowel resection was performed [6].
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.
DATA AVAILABILITY
Data sharing is not applicable to this article as no new data were created or analysed in this study.

{kind=link}
{kind=link}