





Abstract
Arcuate line hernias are a rare type of hernia with limited publications regarding their successful repair. The arcuate line is the inferior limit of the posterior leaf of the rectus sheath. An arcuate line hernia is a type of intraparietal hernia, meaning it is not a truly complete fascial defect of the abdominal and, therefore, may present with atypical symptoms. Although published data on arcuate line hernia repairs are limited to a handful of case reports and one literature review, reports regarding robotic repair are exceptionally rare. This case report is the second documented robotic approach to arcuate line hernias known to these authors.
INTRODUCTION
Arcuate line hernias are a rare type of hernia with limited publications regarding their successful repair. The arcuate line is the inferior limit of the posterior leaf of the rectus sheath. An arcuate line hernia is a type of intraparietal hernia, meaning it is not a truly complete fascial defect of the abdominal and, therefore, may present with atypical symptoms [1]. These hernias are commonly mistaken as Spigelian hernias. As of now, there has yet to be an established standard for the repair of arcuate line hernias. The few published case reports regarding arcuate line hernias describe the repair using both open and laparoscopic techniques. Although a previous case reported a robotic repair of a bilateral arcuate line hernia, there is still very limited existing data.
CASE PRESENTATION
A 72-year-old female with a past medical history of arthritis, fatty liver, hypercholesterolemia, hypertension, a left ovarian cyst and pre-diabetes with a BMI of 25.29 kg/m2 presented with a bulge in her left lower abdomen. Patient had not previously undergone any abdominal surgeries. Abdomen was benign other than bilateral palpable masses. The left-sided bulge was more prominent than the right. CT of the abdomen and pelvis revealed a sizeable Spigelian hernia in the left lower quadrant, with a fascial defect of 3.6 cm with small bowel loops protruding through the hernia defect. The CT also identified a smaller right lower quadrant Spigelian hernia without any involved bowel. The patient was advised to undergo robotic repair of the bilateral Spigelian hernias with mesh.
The procedure was performed using the DaVinci Xi Surgical System. Patient was positioned supine on the operating table. Using a 5-mm trocar under direct vision, the abdomen was entered in the left upper quadrant. Three 8-mm robotic ports were then placed, two fingerbreadths below the left and right costal margin, respectively, and one port subxiphoid. The patient cart of the surgical system was docked from the patient’s right with the anatomy selection set to pelvic. Intraoperative findings revealed the presence of bilateral Spigelian hernias and the incidental finding of bilateral arcuate line hernias and inguinal hernias (Fig. 1). Using the fenestrated bipolar and monopolar scissors, the contents of the hernias were reduced. A preperitoneal flap was developed starting above the arcuate line to include the arcuate line defects and continued caudally to include the Spigelian and inguinal regions. The hernia sacs were reduced. The myopectinal orifice was cleared in its entirety bilaterally. Bilateral round ligaments were divided. The Spigelian hernias on both the left and right sides were identified and primarily closed with absorbable running V-Loc sutures bringing together the two edges of the fascia. The arcuate line hernias were repaired with a running 0 V-Loc suture as follows: the elements of the posterior sheath above the arcuate line (posterior lamella of the internal oblique, aponeurosis of the transversus abdominis, and transversalis fascia) were reattached to the transversalis fascia below the arcuate line to reestablish the normal anatomy and obliterate the hernia defect. An extra-large mid-weight Bard 3D max was then placed over both the right and left myopectineal orifice and secured in place with Vicryl sutures. Subsequently, an 8 × 15 cm soft Prolene mesh was placed beneath the arcuate line hernia repair as an underlay mesh. The peritoneal flap was then closed with a non-absorbable V-Loc suture so that all mesh was completely covered by peritoneum. The preperitoneal space was desufflated with the assistance of an Angiocath ensuring the closure of the peritoneal flap was airtight and complete. The robot was then undocked, and the abdomen was closed in the normal fashion. Total operative time was approximately 3 hours. The patient was discharged the same day, and her post-operative course was uncomplicated.
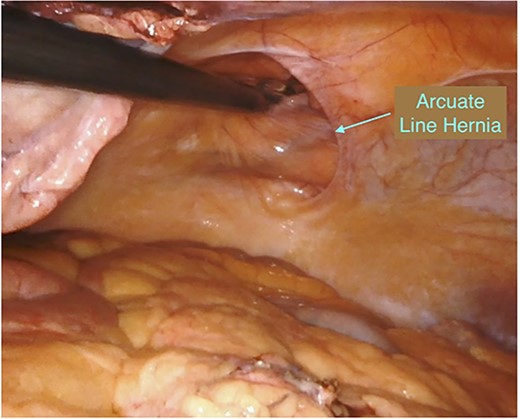
Intraoperative incidental finding of bilateral arcuate line hernias.
DISCUSSION
The arcuate line, or semilunar line of Douglas, is located approximately one-third the distance between the umbilicus and the symphysis pubis. It occurs at the point where the posterior lamella of the internal oblique and aponeurosis of the transversus abdominis transition from contributing fibers to the posterior sheath and instead pass anterior to the rectus muscle contributing to its anterior sheath. Cranial to the arcuate line, the posterior sheath is comprised of fibers from the aponeurosis of the transversus abdominis and the posterior lamella of the internal oblique (Fig. 2). Below the arcuate line, the posterior layer is composed only of transversalis fascia (Fig. 3). Hernias often occur at fascial edges or points of transition, and as such, the arcuate line is a point of potential herniation. In this instance, the herniation may occur at the arcuate line into the potential space between the transversalis fascia and remaining elements of the posterior sheath (aponeurosis of the transversus abdominis and posterior lamella of the internal oblique). Alternatively, the herniation may occur at the arcuate line into the pre-transversalis fascial plane if the transversalis fascia is disrupted at the arcuate line (Figs 4 and 5). As the herniation occurs into the layers of the abdominal wall, it is classified as an intraparietal hernia.
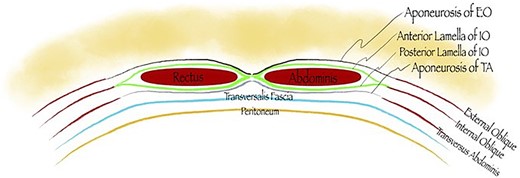
Posterior sheath is comprised of fibers from the aponeurosis of the transversus abdominis and the posterior lamella of the internal oblique (cranial to the arcuate line).
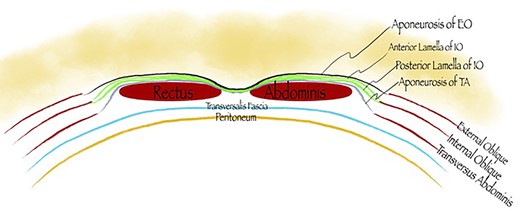
Posterior layer is composed only of transversalis fascia (below the arcuate line).
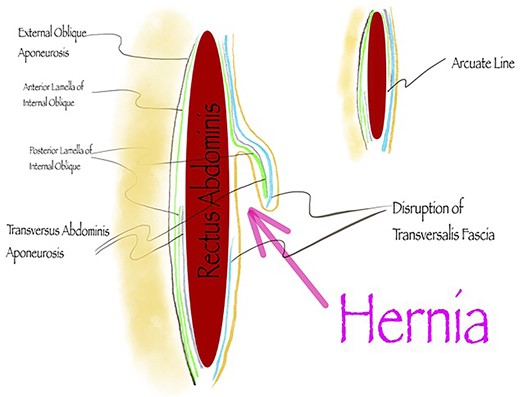
Herniation at the arcuate line into the pre-transversalis fascial plane.
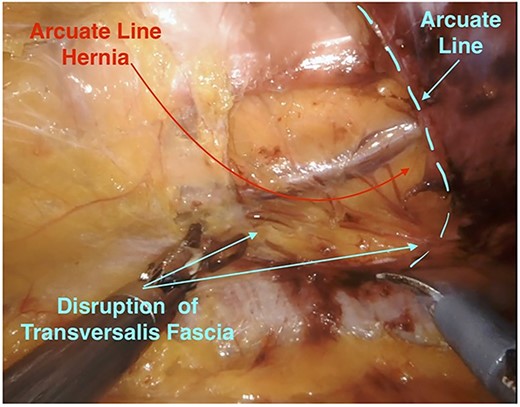
Arcuate line hernia (intraoperative view).
Arcuate line hernias are rare and are often misdiagnosed or found incidentally during laparoscopy. They may be completely asymptomatic. They may also present as an obscure cause of vague, intermittent abdominal pain. Reports of acute incarceration or strangulation are rare in the literature, likely due to the large hernia orifice. Diagnosis can be made on preoperative imaging. CT imaging demonstrates separation of the posterior sheath from the rectus abdominis at the arcuate line with herniated fat or viscus and is best seen on sagittal imaging (Fig. 6).
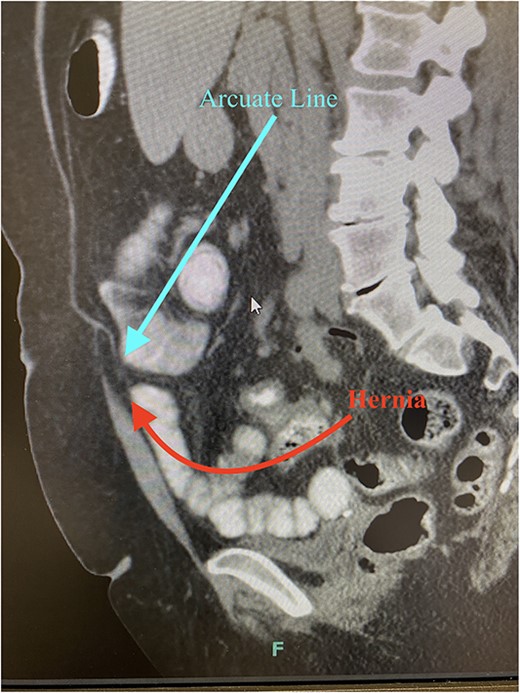
CT imaging demonstrates separation of the posterior sheath from the rectus abdominis at the arcuate line with herniated fat or viscus (sagittal imaging).
There is currently no consensus regarding surgical repair of arcuate line hernias. It is imperative to become familiar with this rare condition to continue improving and innovating the standard of care delivered to patients. Previously, the most common approach to arcuate line hernia repairs was open and laparoscopic techniques [2, 3]. Robotic surgical approaches are popular in the field of general surgery [4]. The robotic platform offers improved visualization, manual dexterity and ergonomics over traditional laparoscopy. This case report is the second documented robotic approach to arcuate line hernias known to these authors.
CONCLUSION
Arcuate line hernia repairs reports regarding robotic repair are exceptionally rare. Robotic repair is a well-documented and well-accepted approach with similar outcomes to those seen in laparoscopic approaches. This approach is likely safe to be extrapolated to arcuate line hernias. In the experience of these authors, the robotic approach was used to repair a right arcuate line hernia successfully and with ease during a procedure in which multiple other abdominal wall hernias were repaired. This approach needs further study, but in our opinion can be a valuable approach consideration, especially in the setting of planned robotic repair of other abdominal wall hernias.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}