





Abstract
A 62-year-old woman presented with 3 months of progressive fatigue without fever or flank pain. Brain natriuretic peptide (BNP) levels were markedly elevated (12 000 pg/mL), with normal C-reactive protein and procalcitonin levels. Chest radiography revealed a cardiothoracic ratio of 61%, and echocardiography revealed severe left ventricular systolic dysfunction with an ejection fraction of 24%. Computed tomography demonstrated bilateral impacted ureteral stones with severe hydronephrosis. Retrograde ureteral stenting was unsuccessful because the contrast agent failed to pass through the stones, and staged bilateral percutaneous nephrostomies were performed. Symptoms rapidly improved after renal decompression. Three months later, the cardiothoracic ratio improved, and the ejection fraction had recovered to 73%, while BNP gradually decreased and normalized by 4 months. No infectious episodes occurred during this period. Thus, non-infectious bilateral urinary obstruction can cause profound but reversible cardiac dysfunction through volume dysregulation or neurohumoral activation, and early decompression may prevent prolonged impairment.
Introduction
Urinary tract obstruction is generally considered a localized urological disorder, whereas urinary tract infections (UTIs) are well known to cause reversible cardiomyopathy or septic cardiogenic shock through systemic inflammation [1–4]. In contrast, the cardiovascular consequences of non-infectious ureteral obstruction remain poorly understood. To date, no reports have documented marked recovery of both left ventricular ejection fraction (LVEF) and brain natriuretic peptide (BNP) levels after relief of asymptomatic bilateral impacted ureteral stones without infection. Here, we report a rare case in which percutaneous nephrostomy alone resulted in profound but fully reversible left ventricular systolic dysfunction, highlighting a previously underrecognized systemic effect of silent obstructive uropathy.
Case report
A 62-year-old woman presented with a 3-month history of progressive fatigue. She had no significant medical history and denied fever, flank pain, or urinary symptoms. On admission, her blood pressure was 182/133 mmHg, heart rate 120 bpm, and SpO₂ 97%. Laboratory testing revealed a markedly elevated brain natriuretic peptide (BNP) level of 12 000 pg/mL, while inflammatory markers were within normal ranges (C-reactive protein, 0.2 mg/dL; procalcitonin, 0.03 ng/mL). Serum creatinine was mildly elevated at 1.44 mg/dL. Chest radiography demonstrated cardiomegaly with a cardiothoracic ratio (CTR) of 61% (Fig. 1a).
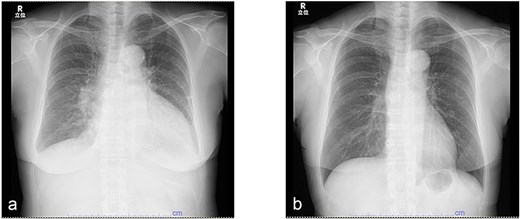
Serial changes in chest radiography. (a) Chest radiograph at initial presentation showing cardiomegaly with a cardiothoracic ratio of 61%. (b) Follow-up chest radiograph after 3 months demonstrating marked improvement in cardiac enlargement.
Transthoracic echocardiography showed severe left ventricular systolic dysfunction with a left ventricular ejection fraction (LVEF) of 24% by Simpson’s method (Fig. 2a). Kidney–ureter–bladder radiography and computed tomography performed to investigate systemic causes revealed severe bilateral hydronephrosis due to bilateral impacted ureteral stones (left: 17 × 7 mm; right: 10 × 8 mm; attenuation ~1350 HU) (Fig. 3). Retrograde ureteral stent placement was attempted on the same day but failed because contrast medium could not pass through the obstructed segments (Fig. 4). A left percutaneous nephrostomy (PCN) was therefore performed, followed by right PCN one week later. Concomitantly, guideline-directed heart failure therapy was initiated, including spironolactone (12.5 mg/day), empagliflozin (10 mg/day), sacubitril/valsartan (100 mg/day), and bisoprolol fumarate (1.25 mg/day).
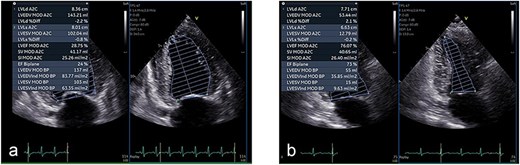
Echocardiographic improvement after urinary decompression. (a) Initial transthoracic echocardiogram showing severely reduced left ventricular systolic function with a Simpson’s ejection fraction (EF) of 24%. (b) Repeat echocardiogram at 3 months showing significant recovery, with EF improved to 73%.
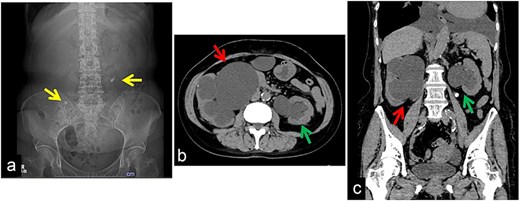
Initial kidney, ureter, and bladder (KUB) and computed tomography (CT) findings. (a) KUB on admission showing a right ureteral stone in the pelvic region and a left ureteral stone in the upper ureter (U1). (b) Axial CT image demonstrating marked bilateral hydronephrosis. (c) Coronal CT image confirming severe bilateral hydronephrosis.
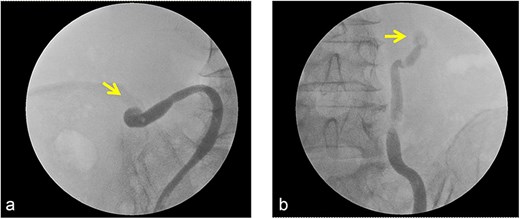
Intraoperative findings during attempted ureteral stenting. Retrograde pyelography demonstrated no passage of contrast agent across the site of the impacted ureteral stone, rendering ureteral stent placement unsuccessful.
After urinary decompression, heart failure symptoms rapidly improved. At 3 months, BNP had decreased to 212 pg/mL, and LVEF had recovered to 73% (Fig. 2b). The CTR normalized, and body weight decreased by 9.2 kg (Fig. 1b). No infectious complications occurred, and antibiotics were not required. After stabilization of cardiac function, endoscopic treatment of the left ureteral stone was performed 4 months after presentation, achieving stone-free status. The right ureteral stone remained under treatment at the time of reporting; however, bilateral PCN drainage was maintained, and no recurrence of cardiac dysfunction was observed.
Discussion
This case provides two important clinical insights. First, noninfectious and asymptomatic bilateral ureteral obstruction can cause severe left ventricular systolic dysfunction. Second, such dysfunction may be fully reversible after urinary decompression alone, without the need for advanced cardiologic interventions. In our patient, LVEF improved from 24% to 73%, with BNP levels normalizing within 3–4 months.
Reversible myocardial depression is well recognized in sepsis-induced cardiomyopathy (SICM). Previous reports of UTI-associated or Escherichia coli–related septic cardiomyopathy describe rapid recovery of cardiac function following infection control and urinary drainage [1–3]. However, these cases were characterized by overt infection and systemic inflammation, whereas in the present case, inflammatory markers, including CRP and procalcitonin, remained within normal ranges throughout the clinical course. This difference suggests a mechanism distinct from classical SICM [4].
One plausible explanation is chronic hemodynamic stress caused by long-standing bilateral ureteral obstruction. Obstructive uropathy can lead to sodium and water retention, activation of the renin–angiotensin–aldosterone system, increased preload, and occult volume overload, even in the absence of infection [5]. Notably, myocardial depression has been reported to arise from sustained hemodynamic stress alone, independent of inflammatory pathways [4]. These mechanisms support the hypothesis that bilateral obstruction imposed chronic myocardial strain, resulting in reversible cardiac dysfunction.
Another potential mechanism resembles cardiorenal syndrome type IV, in which chronic renal dysfunction adversely affects cardiac performance. Restoration of urinary flow after percutaneous nephrostomy may have rapidly attenuated neurohumoral activation, explaining the marked reduction in BNP levels and normalization of cardiac size. In addition, standard heart failure therapies may have acted synergistically with urinary decompression. Angiotensin–neprilysin inhibition promotes reverse remodeling and reduces natriuretic peptides [6], SGLT2 inhibitors provide heart–kidney protection independent of glycemic status [7], and bisoprolol improves survival and left ventricular function [8]. These established effects are consistent with the favorable clinical course observed.
To our knowledge, no previous reports have described severe left ventricular dysfunction caused by noninfectious, asymptomatic, bilateral impacted ureteral stones that resolved following urinary decompression alone. Although limited by its single-case design, this report highlights that obstructive uropathy can exert profound systemic effects beyond renal impairment and underscores the importance of timely decompression, even in asymptomatic patients.
Conclusion
This case shows that asymptomatic bilateral impacted ureteral stones can cause severe yet reversible cardiac dysfunction. Urinary decompression via percutaneous nephrostomy resulted in marked improvement in cardiac function and BNP levels despite the absence of infection. Obstructive uropathy should be considered a potential cause of reversible cardiomyopathy, and early decompression may prevent prolonged cardiac impairment.
Conflicts of interest
The authors declare no conflict of interests.
Funding
This study did not receive any specific grant from funding agencies in the public, commercial, or non-profit sectors.
Patient consent
Written informed consent was obtained from the patient for the publication of this case report.

{kind=link}
{kind=link}
{kind=link}
{kind=link}