





Abstract
Congenital urethral stricture is rare. It has been reported in only four sets of brothers. We report the fifth set of brothers. Cases of two brothers aged 23 and 18 years old diagnosed with low urinary tract symptoms are presented. We diagnosed an apparently congenital urethral stricture in both brothers. Internal urethrotomy was performed in both cases. Both are asymptomatic after 24 and 20 months of follow-up. Congenital urethral strictures are probably more frequent than we think. We suggest that a congenital origin should be considered if there is no history of infections or trauma.
INTRODUCTION
Urethral stricture is any abnormal narrowing of the anterior or posterior urethra [1]. Most urethral strictures arise from iatrogenic, infectious or traumatic cause. Congenital urethral stricture is rare [1]. It occurs usually at the bulbo-membranous junction or at the posterior termination of the fossa navicularis [1]. Congenital urethral stricture occurring in family members has been reported in few sets of brothers [2–5].
We report two cases of apparently congenital bulbar urethral stricture occurring in two brothers.
CASE REPORT
First brother
A 23-year-old medical student was diagnosed with a long history of decrease urinary stream, urinary spraying, dysuria, poor flow and sensation of incomplete bladder emptying. He had no previous history of urinary tract infection, trauma or urethral catherisation. Uroflowmetry was made and peak flow measured at 5.9 mL/s (Fig 1A). Ultrasound showed increased post-void residual urine volume evaluated to 270 mL (Fig. 1B). Retrograde urethrogram showed a short, tight bulbar urethral stricture (Fig. 1C). Urethroscopy confirmed this stricture, and internal urethrotomy was performed and urethral catheter was left for 5 days. A follow-up at 24 months showed no recurrence and the patient was asymptomatic.
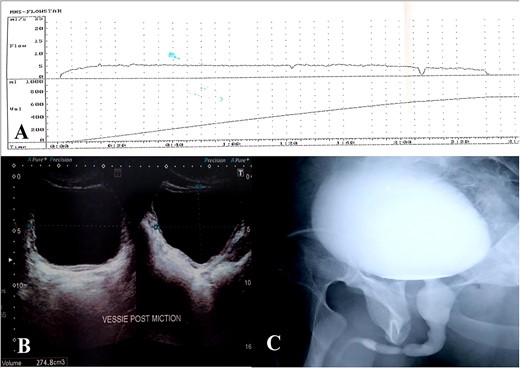
(A) Uroflowmetry, (B) bladder ultrasound, (C) utrethro-cystogram.
Second brother
The 18-year-old brother has been complaining of dysuria and reduced urinary stream in a 5-year duration. He had no history of urinary tract infection, trauma or urethral cauterisation. Uroflowmetry showed decreased peak flow measured at 7 mL/s. Retrograde Urethrogram showed a short tight urethral stricture similar to his brother (Fig. 2A). Urethroscopy confirmed the diagnosis and internal urethrotomy was performed (Fig. 2B). Urethral catheter was left for 5 days. A follow-up at 20 months showed no recurrence and the patient remained asymptomatic.
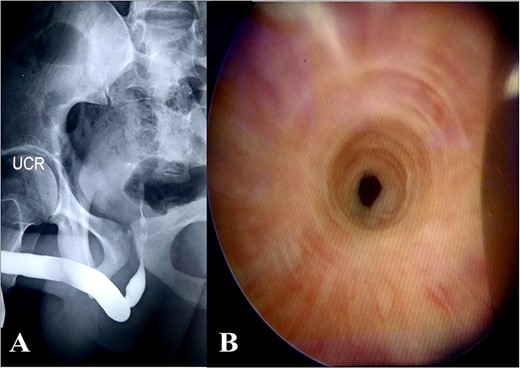
(A) Urethrogram, (B) urethroscopy.
DISCUSSION
Congenital stricture of the posterior urethra is rare and has been reported in only few papers [2–5]. The most commonly accepted explanation is embryological [1]. Cranston et al. explain that in a male, the urethra forms by joining the cloacae (that gives membranous urethra) with the bulbar urethra (which arises from genital folds). The incomplete rupture of the cloacal membrane causes the stricture [1]. It also may be a narrowing in the urogenital ostium located at the level of the opening of the pelvic part into the phallic part of the urogenital sinus (Fig. 3) [1]. In our case, the presence of similar stricture in two brothers who had no previous history seems to indicate a congenital etiology.
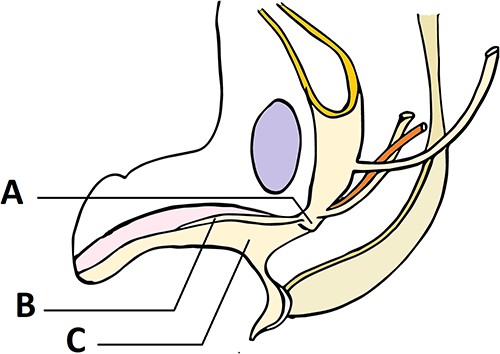
Development of urogenital sinus as explained by Cranston et al. in a 40-mm fetus: (A) pelvic portion of urogenital sinus, (B) line of attachment of urogenital membrane before it disintegrates, (C) phallic portion of urogenital sinus.
Congenital urethral stricture is not commonly diagnosed. The stricture is usually considered as an infectious or long-forgotten traumatic etiology. The age of diagnosis generally reflects the severity of stricture and the majority of patients are diagnosed in their 20s [2–5].
Treatment of these congenital urethral strictures is similar to other urethral strictures. Internal urethrotomy is usually sufficient [2–4]. Urethral dilatations can be done to maintain the diameter [4]. Recurrences can be managed by repeat internal urethrotomy or urethroplasty [4, 5]. In some cases, patients had urethroplasty as the first treatment [5]. In our case, internal urethrotomy was sufficient because the peri-urethral tissues were normal with no apparent fibrosis.
CONCLUSION
Congenital urethral strictures are probably more frequent than we think. When it occurs in the same family members, it is easy to think about congenital etiology. We suggest that a congenital origin should be considered if there is no history of infections or trauma.
CONFLICT OF INTEREST STATEMENT
The authors declare that there are no conflicts of interest regarding the publication of this article.
FUNDING
No funding was received.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The approval of the current study has been granted by the medical committee of research ethics of Charles Nicolle Hospital. Written informed consent was obtained from the patients for publication of this study. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
CONSENT FOR PUBLICATION
Written informed consent was obtained from the patients for publication of this study. A copy of the written consent is available for review by the Editor on request.
CONSENT
Signed consent was obtained from the patients.

{kind=link}
{kind=link}
{kind=link}