





Abstract
Inadvertent ingestion of foreign bodies is a common condition within clinical practice. It rarely produces any symptoms. The diagnosis is difficult since most patients do not recall having swallowed any object. Needles, pins, keys, nails and bones are among the most commonly ingested foreign bodies. Severe complications are uncommon, but if present they can put patients’ lives at risk. Although extremely rare, the ingested foreign body may end lodging in the appendix, posing a challenge for the clinical team. Once the exact location of the object is confirmed, the extraction of the foreign object must be performed to avoid complications. The present report describes a case of a young adult patient, who presented to the emergency room after a routine medical examination. A 30 mm metallic nail was discovered in the tip of the appendix. After a failed endoscopic approach an appendectomy was performed, and the patient underwent a complete recovery.
INTRODUCTION
Ingestion of a foreign body is a common condition in clinical practice. Most cases occur in children, but anyone can be affected. Ingested foreign bodies usually do not cause complications and pass spontaneously through the gastrointestinal tract [1, 2]. However, if a sharp or pointed body is ingested, perforation, bleeding and other complications may occur [2, 3]. The appendix is an unusual site to find a foreign body. Following identification of the location of the ingested foreign body, surgical treatment for the extraction of the foreign body, is required most of the times [2].
We present a case of a 27-year-old male patient. He was completely asymptomatic and did not recall swallowing a sharp object. After proper evaluation and surgery, the patient completely recovered. A 30 mm metallic nail was removed from his appendix.
CASE REPORT
Patient is a 27-year-old male without past medical history. During his annual routine medical examination, an abdominal X-ray was requested. A metallic foreign body (30 mm nail) was discovered in his lower right abdomen (Fig. 1A). With these findings, he was transferred to our hospital. On arrival, he was completely asymptomatic, and he had no recollection of having swallowed the nail. Abdominal examination was unremarkable, and he had no evidence of any surgical scars. With these findings, a contrast-enhanced abdominal computed tomography (CT) revealed the presence of a 30 mm metal nail inside his appendix (Fig. 2A). The appendix had an outer diameter of 5 mm and was surrounded by homogeneous, non-inflamed fat and contained intraluminal air (Fig. 3A). A colonoscopy was requested to assess the cecum to try to remove the foreign body, however, after reaching the cecum and the appendix the nail could not be found (Fig. 1B). An intraoperative abdominal x-ray was needed, which confirmed the presence of the nail in the appendix (Fig. 2B).
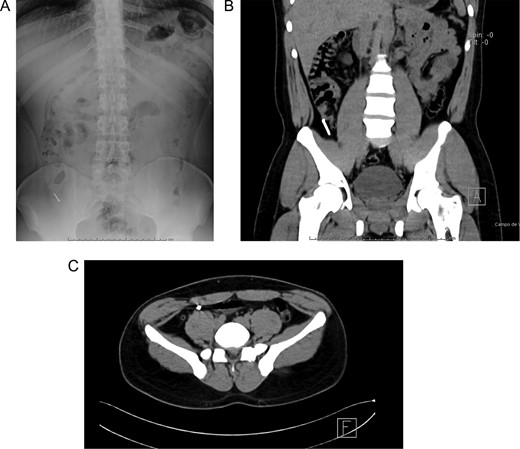
(A) Abdominal X-ray with a radiopaque metallic foreign body. (B) Abdominal CT, the metallic foreign body is lodged in the appendix. (C) Abdominal CT, the appendix is surrounded by homogeneous non-inflamed fat and contains intraluminal air.
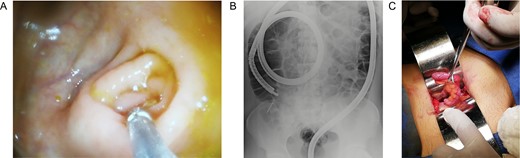
(A) Colonoscopy, the appendiceal orifice is seen without the foreign object. (B) Intraoperative abdominal x-ray confirming the presence of the nail in the appendix. (C) Appendix during surgery.
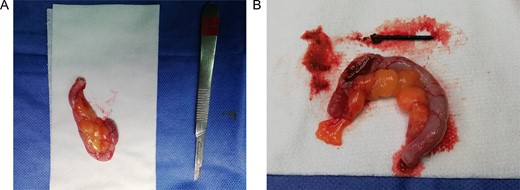
(A) Completely resected appendix. (B) Appendix and metallic nail.
In this context, a surgical approach was needed to assess the appendix and the cecum wall. After a Rocky-Davis incision, the appendix was exposed and an object of hard consistency was found at its tip (Fig. 3B). The surgical decision was straightforward, the appendix was resected, and the surgery was completed without complications (Fig. 1C).
After this, the appendix was dissected and a 30 mm nail was found inside its lumen (Fig. 2C and Supplementary Video).
His postoperative course was uneventful, and he was discharged after full diet was tolerated. In follow-up controls the patient is doing well, and he still has no memory of ever swallowed the nail.
DISCUSSION
Accidental swallowing of foreign bodies is a common condition in clinical practice [1, 2]. Most of them transit through the gastrointestinal system and are passed with the stools without the need of surgical intervention [3]. This happens more commonly among children but anyone can be affected [4]. However, bowel perforation or obstruction, although rare, can still result based on the object size and shape [3]. Identifying a foreign body inside the appendiceal lumen is extremely rare, it only happens in 0.005% of the cases. This occurs when the weight of the foreign body is greater than the bowel fluid, causing it to, halt in the cecum during transit, and finally entering the appendiceal lumen [1, 5, 6]. This depends on the position of the appendix and whether its orifice is obliterated, tight or wide open. Once in the appendix, the object may not be able to re-enter the colon due to a lack of peristaltic action and may cause appendicitis or perforation depending on its morphological characteristics [1, 2]. Round bodies have a low risk (12%), nonetheless, if the object is thin, sharp or metallic up to 93% of the patients will become symptomatic and 70% of them will show inflammation [2, 4].
Since the first description in the 18th century, of a foreign body that caused appendicitis, more than 250 cases of appendiceal foreign bodies have been described [1]. Metal pins, needles, pellets, hair, seeds, tips of thermometers, razor blades, keys, bone and nails have been found in the appendiceal lumen [1, 2, 6–8]. These foreign objects may increase the risk of appendicitis and perforation and may cause delayed complications such us peritonitis, fistula, adhesion and abscesses [4, 6].
Since foreign bodies in the appendix are rare, management approach remains debated [1, 3]. After ingestion of a potentially hazardous foreign object, there should be an immediate attempt to harvest it via gastroscopy [9]. If this fails, careful follow up consisting of weekly X-rays and constant surveillance is recommended [1]. Computed tomography, could be useful to locate the foreign object’s exact position [5]. If it is found in the appendix or the colon with no clear evidence of perforation, colonoscopy should be performed to remove the object. However, if it fails, surgical treatment is recommended even in asymptomatic patients either by laparoscopic or open surgical approaches [6, 10].
There is a need to increase recognition of the potential dangers of accidentally ingested foreign bodies, as they may account for significant morbidity and mortality. When faced with an appendiceal foreign body, treatment should not be delayed. Surgery should be recommended as an appendectomy has a low morbidity and could prevent these patients from severe complications.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}