





Abstract
Hydatid cyst in pregnancy is a rare condition. Moreover, it is very rare that it is in the soft tissue other than the liver. In this case, there are no data in the literature on treatment options, but only experience in case presentations. We present a patient who had severe pain during pregnancy due to isolated soft tissue hydatid cyst disease in this case report.
INTRODUCTION
Hydatid cyst (HC) disease (hydatidosis or echinococcosis) is a parasitic disease that can be seen in all populations. It is estimated that the prevalence in Turkey is 50 per 100.000 and the incidence is 2 per 100.000. The most common causes are Echinococcus granulosus and Echinococcus multilocularis [1].
Parasites are attached to the intestinal mucosa of animals such as dogs, foxes, wolves. The definitive hosts appear quite healthy. Every stool spreads millions of eggs around. The parasite, with its resistant outer layer, can survive for a long time under different climatic conditions. Ingestion of eggs which are expelled in the faeces of the definitive host provides the larvae grow in the visceral tissue of the intermediate hosts (typically sheep and goats and occasionally humans), particularly in the liver and lungs. After ingesting the cysts, the embryo passes through the duodenal mucosa into portal circulation and usually deposits in the liver [2]. This is why the disease is most common in the liver (75%). Embryos occasionally pass through the systemic circulation through the direct anastomosis between the intestinal system vessels and the caval plexus system (Retzius system), without clinging to the liver sinusoids. Rarely, they can reach other parts of the body by systemic circulation through the lymphatic’s and ductus thoracicus [2]. According to the literature 5–10% of the disease occurs in organs such as brain, heart, bone, soft tissue, peritoneum, spleen, pancreas, kidney [3]. About 2–3% of HC cases reported in the endemic areas are located in the soft tissue that is usually associated with involvement of other solid organs, especially liver. However, in rare cases, it may be a primary lesion in the soft tissue.
HC if appears in pregnancy is a rare condition that usually affects liver. In case of soft tissue HC in pregnancies, there is no clear information in the literature regarding the treatment options and only information in case presentations are available. Here we present a case of isolated HC in soft tissue with severe pain during pregnancy.
CASE REPORT
A 28-year-old and 14 weeks pregnant patient presented to general surgery polyclinic with severe pain on her back and right flank. Physical examination revealed tenderness on right lower quadrant of the abdomen, right groin area and right thigh. Ultrasonographic evaluation revealed a lesion showing hypoechoic 46 × 39 mm mass with heterogeneous wall structure on the iliacus muscle at the level of anterosuperior region of the right crista ilica. In magnetic resonance imaging, this lesion was diagnosed as HC (Fig. 1).
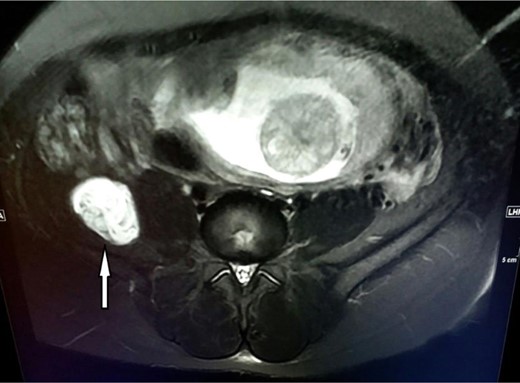
MR imaging of the cystic lesion.
Because of the persistant pain of the patient, she was suggested to have surgery. The patient, lying in the left lateral decubitus position, incised on the mc burney point and the preperitoneal area was reached. This area was dissected towards posterolaterally and retroperitoneum was reached. The cyst was dissected from the adjecent tissues and the iliacus muscle. Posteriorly, the cystic mass was densely adhered to nervus cuteneus femoris lateralis (Fig. 2). It was separated from the nerve by sharp dissections and sent to a histopathological examination (Fig. 3). Histopathologically, it was confirmed that the mass was hydatic cyst. Albendazol treatment was not given to the patient who had not any complaints in postoperative follow-ups. She gave birth at 41th week and there was not recurrence in her 4 years follow-up.
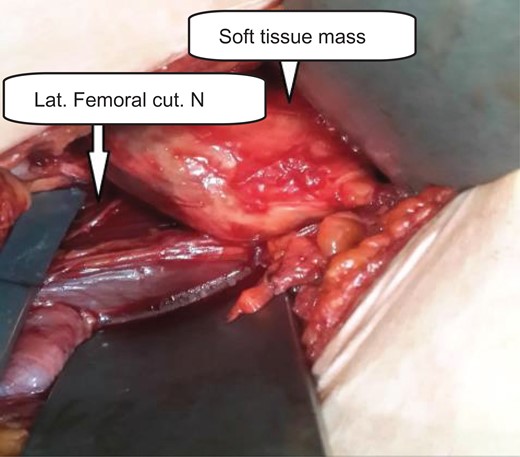
Cystic mass densely adhered to lateral femoral cutaneous nerve; before dissection.

Cystic mass removed.
DISCUSSION
HC is a zoonotic infection that is endemic in Mediterranean countries, Middle East, South America, New Zeland and South Africa. Disease is common in Turkey due to Zoo-geographical structure, climatic conditions, low socio-economic level and inadequacy in veterinary health organization. HC in pregnancy is reported as 1 in 20–30 000 gestations in endemic regions. HC is extremely rare in the skeletal muscle because parasitic cyst growth is inhibited in striated muscle due to muscle contraction and the presence of lactic acid. Intramuscular localized HC disease has been mostly reported in pectoralis major muscle, sartorius muscle, quadriceps and gluteus muscles [4].
Differantial diagnosis
The differentiation of HC in muscle tissue is very difficult and can be mixed with any benign soft tissue tumor [3], particularly abscess, sebaceous cyst, lipoma, fibroma, hematoma and sarcomas should be considered in the differential diagnosis.
Diagnosis
USG, CT and MR are diagnostic radiographic imaging methods. Verification of pre-operative diagnosis is important for anaphylactic shock and local spreading that may occur in the event of rupture [5]. Danice et al. [6] have reported that MR is much more valuable, with USG and BT being although effective in diagnosing intramuscular HC.
Immunologic methods (ELISA) and indirect hemagglutination (IHA) assays can be used besides radiological methods. General serologic tests are useful for diagnosis, but serologic tests in subcutaneous HC are reported to be only 21% positive [7] reported that serological tests were not useful in cases of intramuscular HC disease.In our case serologic tests were negative. USG and MR were used for diagnosis.
Treatment
HC disease has three treatment modalities. These are systemic drug therapy, surgery and percutaneous treatment [PAIR] (percutaneous aspiration, injection, reaspiration). However, surgical treatment is the first choice among these. In uncomplicated HC if there are a large number of cysts, in the cases where surgical treatment cannot be tolerated and when the operation is not accepted; drug treatment is applied. The drug that should be selected at this stage is albendazole
HC in pregnancy
During pregnancy, HC may grow due to suppression of cellular immunity and steroids secreted from the placenta. The cyst can reach a huge volume and may be ruptured. Cyst rupture can lead to deterioration of the general condition of the patient, anaphylactic shock and bleeding [1]. There is very little data available about the treatment, follow-up and complications of HC disease in pregnancy. A small number of cases with CH in liver or lung during pregnancy have been published in the literature [8]. In the early period, cyst excision with surgical operation is the preferred treatment strategy. However, during pregnancy, the operation also has some difficulties.
Percutaneous treatment is not recommended for soft tissue HC because the cysts are usually multiloculated [7]. However, Iyilikci and her colleagues treated a 16-week pregnant patient with liver HC percutaneously who did not had any complication. Sahin and his colleagues treated a 19 weeks of pregnant patient with HC in liver and pelvic region with laparotomy [9]. In another case, a 38-week pregnant patient with hepatic and cardiac HC was operated after the patient gave birth [10]. We preferred surgical treatment because of the proximity of the HC located in the soft tissue to the nervus cutaneus femoris lateralis and the complaints of pain and drowsiness due to pressure. We observed that the cyst is located on the lateral nervus cutaneus femoris and presses on the nerve. In the postoperative period, there was a dramatic decline in the patient’s pain complaint.
During the surgical procedure, care must be taken to remove the integrity of the tissue without deterioration. In many cases, it is possible that the localized masses in the soft tissue can be totally removed. If total removal of the mass is unlikely, drainage should first be irrigated with intra-cystic hypertonic saline solution and then expelled. Particularly, biopsy or puncture for diagnostic purposes or disintegration during removal of the cyst may cause the disease to spread to the tissues and cause anaphylactic reaction [2]. If cyst rupture or contamination of tissues during surgery happens, additional treatment with albendazole should also be started.
The use of antihelmintic drugs in pregnancy as a medical treatment is relatively contraindicated. The use of antihelmintic agents in the first trimester may cause teratogenic effects, but can be used safely in the second and third trimester. In animal studies, these drugs were found to have teratogenic effects in the early period of pregnancy [8]. In the context of this information, we have not used antihelminthic until after the pregnancy has ended.
CONCLUSION
Isolated HC in soft tissue during pregnancy is very rare. Surgical treatment can be safely performed in symptomatic cases. The best time for surgery is the second trimester.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}