





Abstract
A 61-year-old man presented via the emergency department with a few days history of abdominal and colic occlusion symptoms. He presented signs of sepsis, midline lumbar spine tenderness and reduced hip flexion. Computer tomography of the abdomen and pelvis showed a presacral collection contiguous with the posterior part of the colo-rectal anastomosis, and MRI lumbar spine revealed abscess invation into the epidural space. He underwent a laparotomy with washout of the presacral abscess and a colostomy with a prolonged course of intravenous antibiotic therapy. At 3 weeks after initial presentation he had made a full clinical recovery with progressive radiological resolution of the epidural abscess. The objective of the case report is to highlight a unique and clinically significant complication of a rare post-operative complication after rectal surgery and to briefly discuss other intra-abdominal sources of epidural abscess.
Introduction
This was a very unusual presentation of a post-operative complication after rectal surgery. This presentation necessitated early and aggressive surgical and medical treatment to avoid major complications of sepsis. In this case the patient had had a rectal surgery 2 years before that disrupted normal pre-sacral and retroperitoneal anatomy.
Case report
A 61-year-old man presented to the emergency department for fever since few days with abdominal pain and lack of gas and stools. The pain had become worse and was associated with electric shocks in both lower extremities. Two years before, the patient had a laparoscopic proctectomy with ileal pouch–anal anastomosis protected by an ileostomy for a voluminous villous tumor of the lower rectum. This intervention was complicated at the third day of a fever that prompted an abdominal Computer tomography (CT)-scan revealing intra-abdominal effusion in the left flank drained by the per-operative Blake drain, syringed daily and treated by intravenous antibiotics.
The patient had a high fever (T°C 39.3°C) but had no sign of severe sepsis (heart rate was 88 bpm and blood pressure was 113/78 mmHg). The abdomen was painful in the lower median and lower left quadrant. Rectal examination was normal. Neurological examination found still diffuse electric shocks in both lower extremities. The remainder of the full neurological examination was normal.
Blood test revealed elevated inflammatory markers (white cell count 21.49 g/L, C reactive protein 359 mg/L, Fibrinogen 7.4 g/L). An abdominal CT-scan showed a recurrence of digestive tumor in pelvis with a digestive presacral fistulization without circumscribed fluid collection. A sagittal section abdominal CT and magnetic resonance imaging (MRI) (Figs. 1–2) showed colic fistula to the presacral collection measured to 38.8 × 9.54 mm with infiltration of adjacent soft tissue and which continues to the spinal canal through the sacral S1 left hole with multiple epidural abscess from L4 to S4. There was osteitis of the sacrum and arachnoiditis.
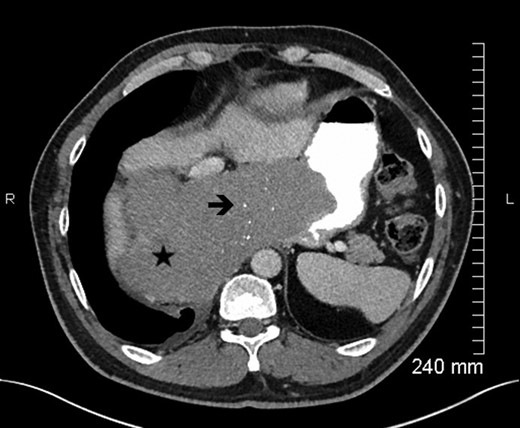
Axial view contrast-enhanced MDCT (portal phase) with oral opacification, in a x year-old men with a large esophageal GIST, showing a lesion (★), well-circumscribed, with small calcifications (è) (rare). The lesion is homogeneous (no kystic or necrotic parts) without hypervascularization.

Coronal view of contrast-enhanced MDCT showing the exophytic, non-obstructive lesion (★) located at the esogastric junction.
The patient underwent a new surgery by laparotomy. An intraoperative rectoscopy was performed. At the joining up end-to-end anastomozing colon, there was a hole that may correspond to a fistula orifice. A colostomy was performed to defunctionalize the fistula. On consultation with the microbiology treatment, an empiric intravenous antibiotic therapy was started by Piperacillin–Tazobactam with Amikacin and Metronidazol then switched by Piperacillin–Tazobactam against the septicaemia of Escherichia coli (found in blood culture) during 2 months.
Discussion
Previous studies published about epidural abcess secondary to abdominal sepsis concern a context of appendicitis, stercoral ulcer rupture, immunocompromised patients, acutization of Crohn's disease, disadvantaged social status and bad oral conditions. One study described presacral pelvic abscess continuous with the tip of the appendix in a patient of antecedent of rectal adenocarcinoma. The other one concerns presacral pelvic abscess at the recto sigmoid junction extended into the presacral musculature and gas bubbles extended into the epidural space at L3. However, there are no studies dealing with a presacral fistula between a chronic presacral collection and spinal canal after of laparoscopic proctectomy for tubulo-villous resection of rectum with osteitis and arachnoiditis. It was sometimes necessary to realize intervertebral disc biopsy [1], bacteriological fluid drainage [2], parasitological examination of stools [3] and lumbar puncture [4]. The variation of symptoms depended on neurological involvement and the importance of the fistula. The origin of the abscess was different between cases reported: presacral pelvic abscess continuous with the tip of appendix after abdominoperineal resection for adenocarcinoma and chemo radiotherapy [2], stercoral ulcer rupture[5], immunocompromised patients, acutization of Crohn's disease [5], disadvantaged social status, bad oral conditions [1], fistula after laminectomy L4 between the wound and the first sacral foramen [6]. The abscess concerns more frequently the cervical spine but any spinal cord could be reached and cause a fistula with other soft tissue. There is no precise data in the literature about the time between the abscess and this cause.
In our case, the patient underwent a defunctioning pelvic loop colostomy by laparotomy. An empiric intravenous antibiotic therapy was started to Piperacillin–Tazobactam with Amikacin and Metronidazol then switched by Piperacillin–Tazobactam against Escherichia coli (found in blood culture) during 2 months.
On the one hand, the duration of antibiotherapy was 6 weeks to 6 months in the literature. There is no data in this one about the choice of duration. The choice may be chosen by the degree of clinical neurological and imagery damage as well as the germs found in bacteriological samples.
Negative Gram bacilli were most frequently found especially Bacteroid Fragilis and E. coli and positive Gram bacilli (Streptocoque intermedius). On the other hand, all teams operate their patients except for two case reports of Lechiche et al. in 2006 who decided to use only medical treatment with antibiotics [5]. For the others, decompressed laminectomy was each time necessary in the case of neurological deficit at the clinical examination with a fluid drainage [2, 4]. In our case, as in the M.H. Jamison's case report in 1984, a defunctionning pelvic loop colostomy was necessary [3]. An appendectomy was necessary with a drainage of the collection for the case of Carter et al. in 2014 [2], an urgent Hartmann's resection for focal perforation of the recto sigmoid junction for the case of Uy et al. [7] and ileocecal resection of the affected bowel with drainage of the multiple abscesses in R. Maggiore's Case [4].
Concerning the type of antibiotherapy, there was no consensus and each team used different initial empiric antibiotics. What can be noticed is that after antibiogram most teams used a G penicillin associated with metronidazole. Only one team has chosen to switch with intravenous Piperacillin–Tazobactam [7]. For five of these studies, the evolution has been favorable [2–4, 6, 7]. One death occurred in the published literature [5]. Definitive paraplegia occurred in one case [1]. A resolution of intraspinal gas and abscess but persistent sacral osteomyelitis occurred in two cases [5, 7].
To conclude, this is a very rare affection but it can lead to serious complications. Successful treatment involves prompt drainage and prolonged intravenous antibiotic therapy.
Acknowledgements
We thank Dr Audrey Fohlen, MD-MSc, Radiologist, for the help in the MRI review.
Conflict of Interest Statement
None declared.

{kind=link}
{kind=link}