





Abstract
Angiolipoma is a rare variant of lipoma. Infiltrating chest wall angiolipoma usually presents as painful subcutaneous lesions. There are only a handful of cases reported in the literature. Malignancy is suspected in the differential diagnosis, and hence a tissue diagnosis is needed to rule out an underlying malignancy. Symptomatic infiltrating angiolipoma warrants surgical excision. We report a case of an infiltrating angiolipoma of the chest wall, which was successfully treated with surgical excision.
INTRODUCTION
Angiolipoma is a rare histological variant of lipoma and is considered to be a benign tumour. Infiltrating chest wall angiolipoma is a rare entity. There are only a handful of cases reported in the literature. It presents as painful subcutaneous lesions on the chest wall in young healthy adults. Surgical excision is recommended for both diagnostic and therapeutic purposes [1]. We report the case of a 42-year-old lady who presented with a left posterior chest wall angiolipoma that was treated with surgical excision.
CASE REPORT
A 42-year-old Caucasian lady presented to our services complaining of left posterior chest wall pain that had been ongoing for more than a year. She has a family history of neurofibromatosis type I and is a Jehovah's Witness; otherwise, she has no other relevant past medical history and no personal or family history of tuberous sclerosis. On physical examination, a tender immobile lump was palpated at the left fourth thoracic vertebral level (T4) at the paravertebral gutter.
Magnetic resonance imaging (MRI) scan of her chest showed an infiltrating multi-lobulated soft tissue mass (95 mm × 40 mm × 10 mm) arising at T4 between the third and fourth left intercostal spaces without involvement of any neurovascular bundles (Fig. 1). This mass appeared to be deep to the trapezius, rhomboid major and minor muscles. Pleural thickening was noted at the same region without involvement of the lung parenchyma. The mass was non-fludeoxyglucose avid on positron emission tomography (PET)/computed tomography (CT) scan.
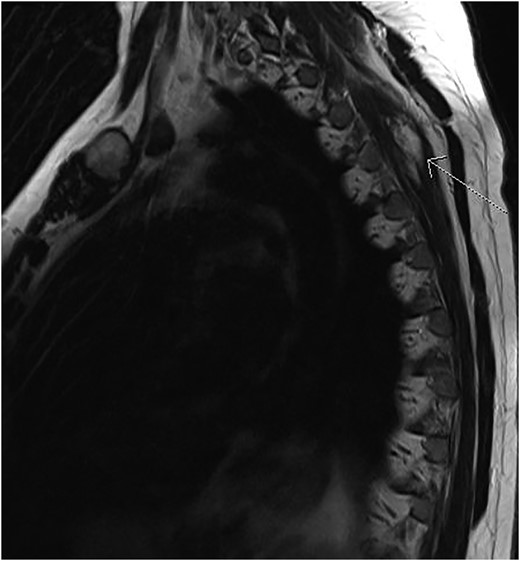
MRI scans shows infiltrating angiolipoma lesion in the left posterior thoracic wall, deeper to trapezius and rhomboid muscles (arrow).
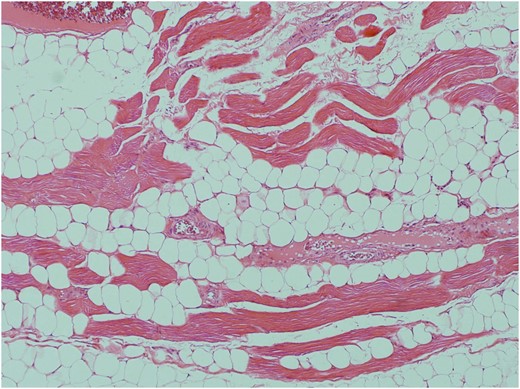
Patient initially underwent a video-assisted thoracoscopic biopsy of this mass in order to rule out an underlying malignancy. Biopsy results showed non-specific adipose cells. After discussion of her case and histology in our institution's multidisciplinary meeting and given that the patient was still complaining of pain around that region, a decision to proceed with surgical excision was made. We performed a wide local excision of the chest wall lesion (Fig. 2), and the patient had an uneventful recovery. Post-operatively, her long-standing neuropathic pain reduced significantly. Histological study of the lesion showed abundant lobulated adipose tissue noted to extend between skeletal muscle fibres. This also incorporated a vascular lesion displaying organizing thrombus formation within occasional vascular lumens (Fig. 3). These findings are consistent with typical features of an angiolipoma.
Macroscopic image of fragmented angiolipoma lesion.

A vascular lesion composed of large thin- and thick-walled blood vessels embedded within adipose tissue. 4× objective under haematoxylin and eosin staining.
DISCUSSION
Angiolipoma is a rare variant of lipoma. It most commonly occurs in the upper extremity and trunk and usually presents with small, painful lesions. Howard and Helwig first reported angiolipoma in the literature in 1960. Histologically, angiolipomas are classified as infiltrating and non-infiltrating. Lin and Lin initially reported this classification in 1974 [2]. In our case report, our patient had an infiltrating angiolipoma invading the external and internal intercostal muscles, without involvement of the parietal pleura.
Angiolipoma has distinct morphological features that consist of mature adipose tissue with numerous small blood vessels, which are capillaries. Also, fibrin thrombi are almost always present. These suggest a different pathogenesis from pure lipoma and are considered to be a benign condition.
Pre-operative diagnosis of an angiolipoma is challenging. Various modalities are described in the literature from a simple ultrasound scan to angiography. These are mainly aimed to differentiate between a simple lipoma and an angiolipoma. MRI scans are preferred specifically to identify the nature of soft tissue lesions and its involvement to the surrounding tissues. Angiographic studies are used to study the extent of vascular involvement. In our case, we used MRI and PET scans mainly to rule out the possibility of an underlying malignancy. Despite an increase in vascularity, angiolipomas showed a minimal increase in metabolism. Chest wall angiolipomas are a rare entity of this tumour.
A search of PubMed revealed that only four chest wall angiolipoma case reports have been published (Table 1). Three out of the four case reports described cases of patients who were asymptomatic adults. One patient had a history of the von Recklinghausen neurofibromatosis. This particular patient had an infiltrating angiolipoma of the chest wall.
Summary of published case reports
| Case summary | Authors | Type | Investigation | Surgery | Complications | |
|---|---|---|---|---|---|---|
| 41 YR M, pain less, soft, posterior-lateral thoroco-abdominal wall mass | Biondetti et al. 1982 [3] | Infiltrating | CT | Surgical excision | Nil | Abstract only |
| 18 YR F, giant angiolipoma of back and chest wall with A-V malformation | Deviri et al. 1987 [4] | Not specified | Not specified | Total (4 stage) excision of the tumour, auto transfusion | DIC and blood loss, recovered eventually | Abstract only |
| 25 YR M, asymptomatic, incidental finding of chest wall tumour | Hamano et al. 2013 [5] | Non-infiltrating | CT scan | Surgical excision | Nil | Full paper |
| 18 YR M, chest pain with history of the von Recklinghausen neurofibromatosis; chest wall angiolipoma | Komatsu et al. 2013 [1] | Infiltrating | CT scan | VATS excision | Nil | Full paper |
DIC, disseminated intravascular coagulopathy; VATS, video-assisted thoracoscopy; YR, year; M, male; F, female.
In conclusion, infiltrating angiolipoma is a rare but potential cause of chest wall pain in young adults. Radiological investigations are helpful to assess infiltration of surrounding tissue and vascularity of the lesion. Surgical excision and histological examination of the lesion are warranted to confirm diagnosis.
Written informed consent was obtained from the patient for publication of this Case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}