





Abstract
Blunt aortic injury is the most lethal injury of the thorax, of which aortic transection is the second leading cause of death. Pseudoaneurysm formation is seen in patients who survive the injury and arrive to the emergency department with small or partial-thickness tears of the aorta. In general, the proximal descending aorta is most commonly afflicted due to the relatively mobile aortic arch moving against the fixed descending aorta. There are several factors associated with a high risk of aortic injury including high-speed motor vehicle collision (MVC) accidents, unrestrained drivers and passengers, extensive impact/collision and abrupt deceleration of motor vehicles. In this case study, a 28-year-old male patient with a thoracic aorta injury is presented. Diagnostic findings consistent with transection and/or dissection and a review of his surgical management are also discussed.
INTRODUCTION
In the USA, up to 15% of all deaths following motor vehicle collision (MVC) are due to injury to the thoracic aorta [1]. Blunt aortic injury is the most lethal injury of the thorax, of which aortic transection is the second leading cause of death [1]. Pseudoaneurysm formation is seen in patients who survive the injury and arrive to the emergency department (ED) with small or partial-thickness tears of the aorta. In general, the proximal descending aorta is most commonly afflicted due to the relatively mobile aortic arch moving against the fixed descending aorta [2]. There are several factors associated with a high risk of aortic injury including high-speed MVC accidents, unrestrained drivers and passengers, extensive impact/collision and abrupt deceleration of motor vehicles. The highest incidence of aortic transection is seen in males aged 21–30 years old [2].
CASE REPORT
A 28-year-old male bicyclist was hit by car and brought to our Level 1 Trauma Center. He had loss of consciousness in the field with a Glasgow Coma Scale (GCS) score of 6. He was intubated for altered mental status. Breath sounds were present bilaterally. Circulation was assessed via physical examination and Doppler US and revealed bilateral lower extremity pulses to be diminished. He sustained left facial and left posterior chest wall abrasions as well as a deformity of the right lower leg with an open tibia fracture. Cardiovascular examination revealed normal heart sounds with a sinus rhythm and clear lung fields bilaterally. Focused Assessment with Sonography for Trauma ultrasound examination was negative for fluid in all four windows.
Chest, pelvis and right lower extremity X-rays were obtained. Chest X-ray findings are shown in Fig. 1. Pelvic X-ray was negative for acute injuries. Right lower extremity X-ray revealed the presence of a right tibia-fibula fracture and the right lower extremity was immobilized with a posterior splint.

Initial chest X-ray.
Vital signs obtained in the ED and initial laboratory findings are as follows: Blood pressure: 156/103; Heart rate: 110; Respiratory rate: 21; Temperature: 98.7F, pH = 7.11; Base deficit = −14; lactate = 6; H-H = 12/37.
Further imaging included CT scans of the brain, cervical spine, abdomen and pelvis. CT angiogram (CTA) of the aorto-ilio runoff was also ordered and initial CTA assessment revealed an aortic intimal flap with a pseudoaneurysm 2 cm distal to the take-off of the left subclavian artery from the aortic arch. Additionally, there was disruption of the medial wall of the descending thoracic aorta findings consistent with transection and/or dissection.
The patient was emergently admitted to Intensive Care Unit for tight control of blood pressure which was titrated within a systolic of 90–100 mmHg with 40 mg IV Cardene.
The patient was taken emergently to the vascular hybrid room where the left common femoral was accessed percutaneously. A 26–21 mm diameter tapered Gore Tag® endograft was positioned at the left subclavian artery and deployed. The pseudoaneurysm was sealed and the transection resolved (Figs 2 and 3).
Following thoracic endovascular aneurysm repair (TEVAR) stent placement, the patient's tibial fracture was fixed and the rest of his hospital course was uncomplicated. The patient was discharged 7 days after admission on PO aspirin.
DISCUSSION
Conventional management of an aortic transection can involve an open surgical or endovascular approach. TEVAR was initially developed to treat those who were not surgical candidates, but in the last decade, this has become a suitable alternative to open surgical techniques. Several recent studies have shown a favourable post-operative outcome for patients who underwent endovascular aneurysm repair for injuries to the thoracic aorta vs. the open surgical repair. One study demonstrated that operative mortality was halved in patients who underwent stent-graft repair vs. the open surgical repair in cases of injury to the thoracic aorta [3]. The researchers also found post-operative complications to be similar between the two groups including similar rates of re-interventions.
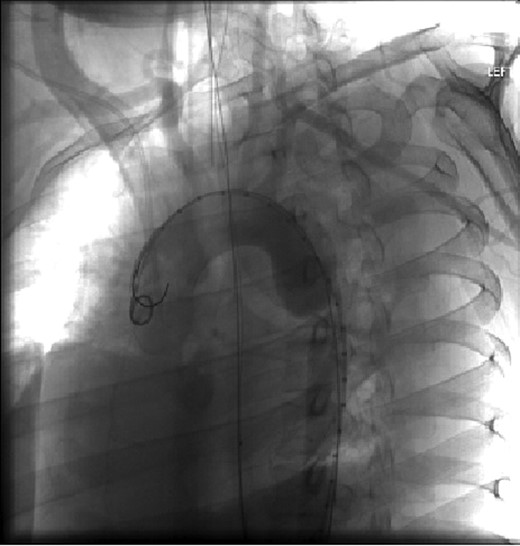
Aortic arch and descending thoracic aorta visualized by CTA with contrast pre-placement of stent.
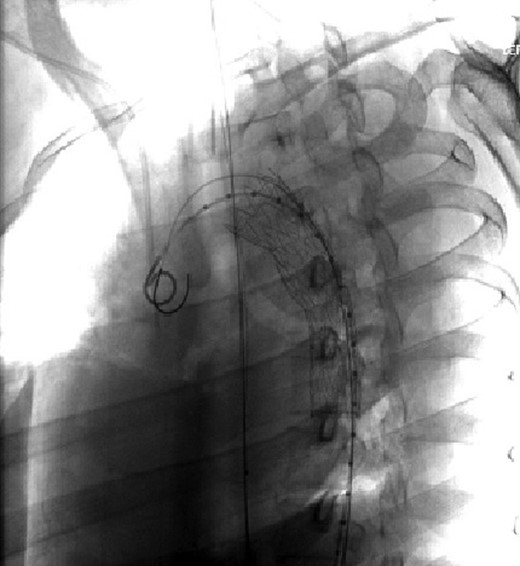
Visualization of the aortic arch and thoracic aorta after stent placement.
In another clinical trial conducted at 42 international sites, the effectiveness of TEVAR with a TX2 endovascular graft was tested in comparison with an open surgical repair post-operatively after 1 year [4]. They were able to demonstrate cumulative major morbidity scores to be significantly (<0.05) lower at 30 days for the TEVAR group compared with the open group. Additionally, they found device performance issues to be infrequent but follow-up with imaging was deemed necessary for all subjects. Additionally, a multicentre trial looked at 140 patients with descending thoracic aorta aneurysms and was able to demonstrate the merits of early endovascular grafting in comparison with those subjects undergoing an open surgical repair [5]. Importantly, the study was also able to demonstrate that there is an incidence of endoleaks and re-interventions associated with endovascular repair at the 2-year follow-up. While early endovascular graft stenting in patients presenting with acute thoracic aorta injury and has shown favourable outcomes, frequent follow-up evaluations of the stent are advised as part of comprehensive post-operative care.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}