





Abstract
Gastric volvulus is a rare condition with two forms of presentation, either acute or chronic. Since its discovery, there have been no cases of acute on chronic volvulus discussed in the literature. Its vague presentation makes diagnosis and subsequent management difficult. The diagnosis of acute gastric volvulus is made on clinical grounds via Borchardt's triad; however, barium swallow and oesophagogastroduodenoscopy have been shown to play a role. We describe a case of a 95-year-old Caucasian woman who presented with worsening dysphagia, epigastric pain, retching without vomiting and hiccups of 5 months. Initially diagnosed as a hiatus hernia, the patient subsequently died following an acute on chronic gastric volvulus. This rare, life-threatening diagnosis provides an opportunity to discuss characteristics of gastric volvulus and the difficulties in management.
INTRODUCTION
Since Borchardt discovered gastric volvulus in 1904, there have been multiple cases of acute volvulus and its management described [1–3]. However, there have been no cases of acute on chronic volvulus reported in the literature.
Over the last 20 years, the incidence and prevalence of chronic volvuli are unknown due to many going undiagnosed and managed as gastro-oesophageal reflux [3–5], which as this case emphasizes can be a life-threatening error.
Paraoesophageal hernias are the commonest cause and the peak incidence occurs during the fifth decade. Our patient was significantly older than this and found to have a chronic volvulus that had passed through the diaphragmatic hiatus. The only symptom that may have indicated the presence of a chronic volvulus was the existence of a history of hiccups [6].
CASE REPORT
A 95-year-old Caucasian woman presented with worsening dysphagia, epigastric pain, retching without vomiting and hiccups over 5 months. Oesophagogastroduodenoscopy (OGD) was unsuccessful due to failed intubation. Fibreoptic nasoendoscopy revealed pooling of saliva in the piriform fossa and a diagnosis of pharyngeal pouch was initially made. Barium swallow was abandoned due to aspiration by the patient (Fig. 1).
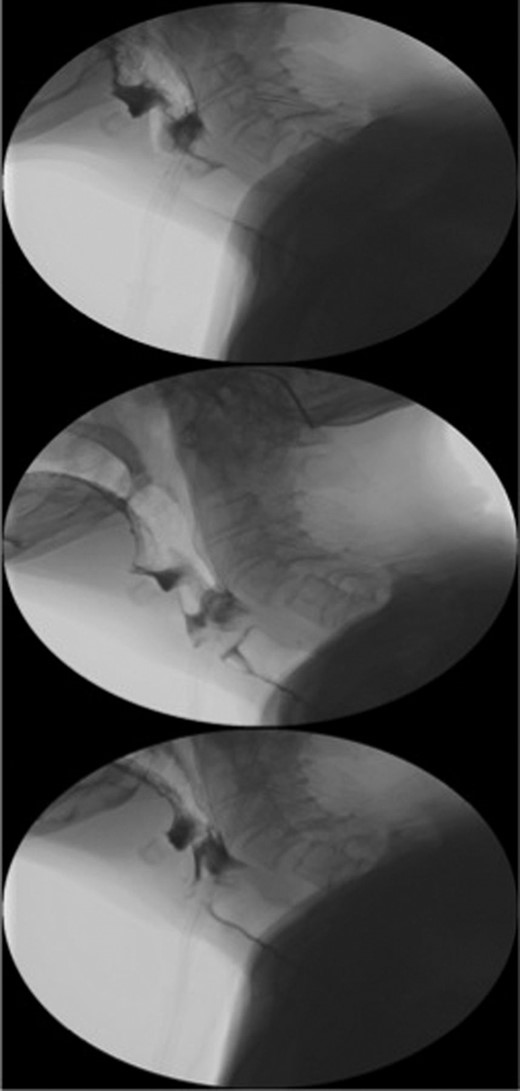
Sequence of barium swallow examinations revealing upper oesophageal tightening and aspiration.
The patient was referred to ENT for endoscopic insertion of a nasogastric (NG) tube as the initial attempt failed. Resistance was noted at 40 cm and failure to pass beyond the lower oesophagus. Chest X-ray revealed the NG tube tip in the distal oesophagus (Fig. 2).

Chest X-ray showing the NG tube blocked at the distal oesophagus. The typical retrocardiac gas filled viscus cannot be seen.
Her symptoms continued to range from severe retching without vomiting with hiccups to intermittent abdominal fullness and dysphagia hence the need for NG tube insertion. Radiographically, there were no features of a volvulus and required a diagnostic OGD. This was abandoned due to the patient condition.
Repeated attempts of NG tube insertion failed due to blockage at the distal oesophagus. A CT scan revealed that an organoaxial volvulus had transmitted through the diaphragmatic hiatus and was occupying the thoracic cavity. No strangulation was noted (Fig. 3). The decision was made to treat the patient conservatively due to the patient's multiple comorbidities and life expectancy.

CT thorax sagittal and coronal views revealed an organoaxial volvulus with the stomach occupying the thoracic cavity. White spot indicating the NG tube tip unable to pass through the volvulus.
DISCUSSION
Gastric volvulus is a rare clinical entity that is defined as an abnormal rotation of the stomach of >180°, leading to obstruction, strangulation and eventual necrosis. Clinical presentation varies from incidental radiographic finding to catastrophic strangulation dependent on the degree of rotation and subsequent extent of strangulation.
Several classification systems exist, anatomical variations including organoaxial, mesenteroaxial or combination of them both, onset of symptoms, acute or chronic (symptoms >3 months) or primary/secondary based on aetiology [7].
Organoaxial is the commonest form of acute volvulus occurring in approximately two-thirds of cases and is commonly secondary to paraoesophgeal hernias [7]. It involves the stomach rotating around an axis that connects the gasto-oesophageal junction and the pylorus with the antrum rotating in an opposite direction to the fundus.
Acute volvulus results in vascular compromise leading to the classical Borchardt's triad of symptoms seen in 70% of cases, severe epigastric pain, retching without vomiting and inability to pass an NG tube. Gastric infarction can lead to acute upper GI haemorrhage, shock and death.
Chronic volvulus presents with abdominal fullness, intermittent epigastric pain and hiccups [6]. The pain and discomfort is similar to peptic ulcer disease, gastritis, cholecystitis or angina. If the gastro-oesophageal junction is distorted, reflux is their main complaint.
Barium swallow is considered the gold standard due to its ability to examine the degree of obstruction and rotation [2, 3, 8]. Endoscopy has been shown to be reliable with difficulty in passing the pylorus being the principal finding [7].
CT scanning can aid diagnosis, but should not delay time to surgery if indicated. In haemodynamically stable patient's endoscopy can confirm a tortuous appearance of the stomach as well as confirm diagnosis via inability to reach the pylorus.
Definitive treatment of gastric volvulus includes reduction of the twisted stomach, percutaneous endoscopic gastrostomy or gastropexy [3]. The treatment of acute volvulus typically involves immediate surgical repair to prevent vascular compromise. Where patient's co-morbidities prevent this, endoscopic reduction has been reported. However, this does not resolve the underlying ligament laxity predisposing to stomach torsion.
Chronic volvulus is often treated conservatively with watchful waiting. However, a recent review of conservatively managed volvuli revealed a high symptom recurrence rate (64%) [5]. None of their cohort developed acute complications over a follow-up period of 69 months.
This case demonstrates the variability in presenting symptoms of acute on chronic gastric volvulus. In stable patients, diagnosis should be via CT scan, following normal chest and abdominal radiography. Patient's co-morbidities and age should dictate surgical intervention or conservative management as transformation into acute volvulus is often life threatening.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}