





Abstract
This case describes a 60-year-old gentleman who presented with a pulsating mass behind his knee. Before this, he had a fasciotomy for suspected compartment syndrome of leg following knee arthroscopy, but this failed to resolve his leg symptoms. He was hemodynamically stable on presentation. His left calf was swollen with a circumference of 3 cm greater than right. There was a large pulsating mass palpable in his left popliteal fossa. Distal neurovascular status of the leg was intact. He had a normal cardiovascular, respiratory, abdominal and neurological examination. Ultrasound showed a cystic mass in the popliteal fossa suggestive of aneurysm. CT angiogram demonstrated a 6 × 5 × 4 cm pseudoaneurysm compressing and displacing the left popliteal artery with satisfactory three-vessel run-off. An emergency repair was performed. An arteriotomy was identified at the proximal end of pseudoaneurysm and it was closed with a patch of small saphenous vein. It led to a good clinical outcome.
INTRODUCTION
Compartment syndrome is a known complication of knee arthroscopy, and so is popliteal pseudoaneurysm. In this case, both of these clinical entities occurred simultaneously. Initially, the compartment syndrome was thought to be a direct result of arthroscopy. However, a fasciotomy did not lead to complete resolution of symptoms, until the patient had definitive treatment of his pseudoaneurysm. This case reminds an important clinical lesson that, in post-surgical swellings, we should always suspect an underlying vascular cause. It also suggests that an early ultrasound should be booked to rule out a pseudoaneurysm hiding underneath an apparent compartment syndrome.
CASE REPORT
A 60-year-old gentleman was referred to the vascular surgery service, from the orthopedics department, with a ‘pulsating mass’ behind the left knee. He had a background medical history of hypertension and hypothyroidism. He was taking candesartan and levothyroxine sodium regularly.
He hit his left knee while getting out of a lorry, 2 months before this presentation. An MRI at that stage confirmed lateral meniscal tear, and there was no other injury to surrounding structures. He had a left knee arthroscopy and repair of meniscal tear after a few weeks. He developed a swollen leg soon after the surgery. With significant swelling of his calf, and pain out of proportion and intracompartmental pressure of 40 mmHg, a clinical diagnosis of compartment syndrome was made and fasciotomy was performed to relieve the pressure in fascial compartments in the leg.
However, he had persistent pain in calf and knee, and after a few weeks, when his calf swelling reduced, a pulsating mass was felt behind the same knee. An ultrasound performed, showing a 7 × 4 cm thick walled cystic mass in the popliteal fossa filled with irregular blood, suggestive of a popliteal aneurysm.
On examination, he was hemodynamically stable. His left calf was swollen with a circumference of 3 cm greater than his right. There was a large pulsating mass palpable in his left popliteal fossa. Distal neurovascular status of the leg was intact. He had an unremarkable cardiovascular, respiratory, abdominal and neurological examination.
His laboratory reports for full blood count, urea and electrolytes were normal. In view of the ultrasound findings, a CT angiogram of lower limbs was performed. It confirmed 6 × 5 × 4 cm pseudoaneurysm, compressing and displacing his left popliteal artery. However, three-vessel run-off below the knee was satisfactory (Figs 1 and2).

CT angiogram of the left leg, coronal section, shows popliteal pseudoaneurysm (asterisk), communicating and displacing the popliteal artery (arrow).
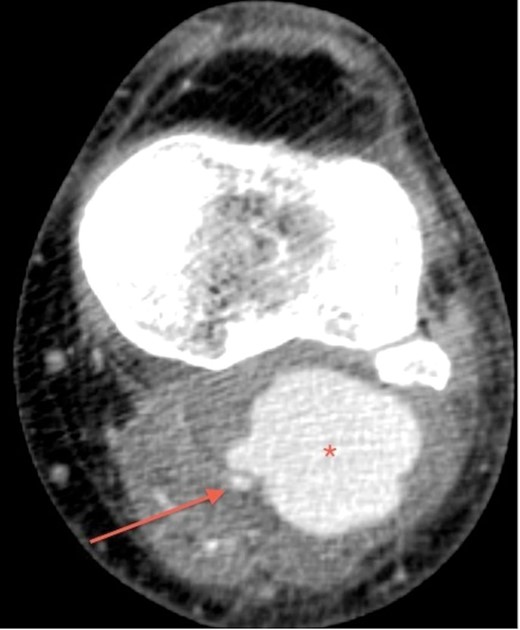
CT angiogram of the left leg, transverse section, shows popliteal pseudoaneurysm (asterisk) adjacent to the popliteal artery (arrow).
A diagnosis of iatrogenic popliteal pseudoaneurysm secondary to arthroscopy was made. The absence of this on his MRI after before his arthroscopy suggests that it was not related to his initial trauma.
Compartment syndrome was considered to be secondary to his pseudoaneurysm due to its pressure effect. The initial significant calf swelling may have masked the clinical findings of a pulsating mass, but as the swelling reduced several weeks post-surgery, the pseudoaneurysm became easily palpable.
An emergency open repair of the popliteal pseudoaneurysm was undertaken. During the surgery, an S-shaped incision was made in the popliteal fossa. Initial dissection was difficult because of the overlying popliteal vein and tributaries. After achieving proximal and distal control, the pseudoaneurysm was opened and clot was evacuated (Fig. 3). The arterial injury was easily identified at the proximal end of the pseudoaneurysm (Fig. 4) and was closed with a patch of short saphenous vein (Fig. 5).
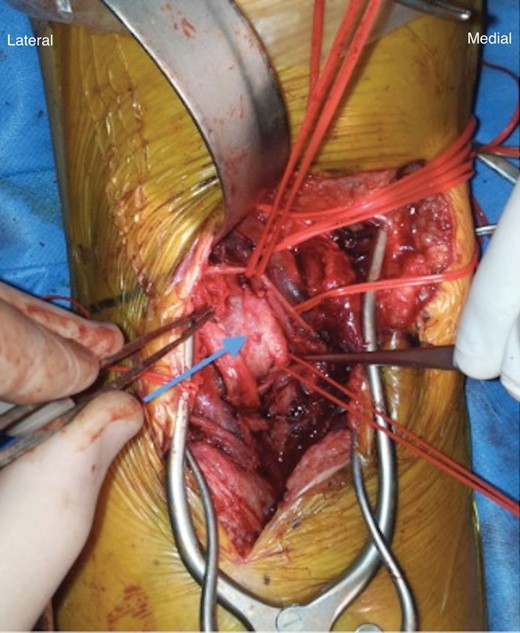
Intraoperative finding of popliteal pseudoaneurysm.
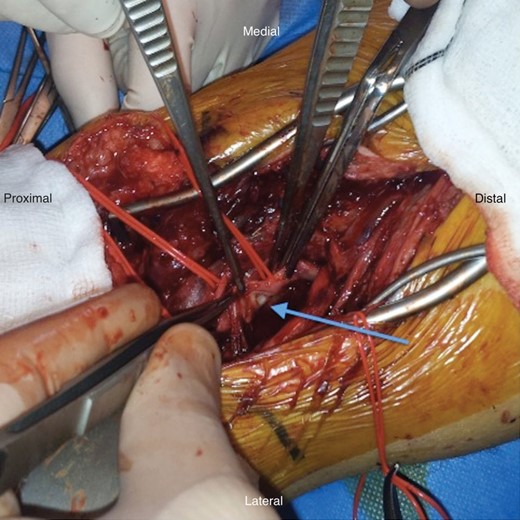
Arteriotomy, after evacuating pseudoaneurysm.
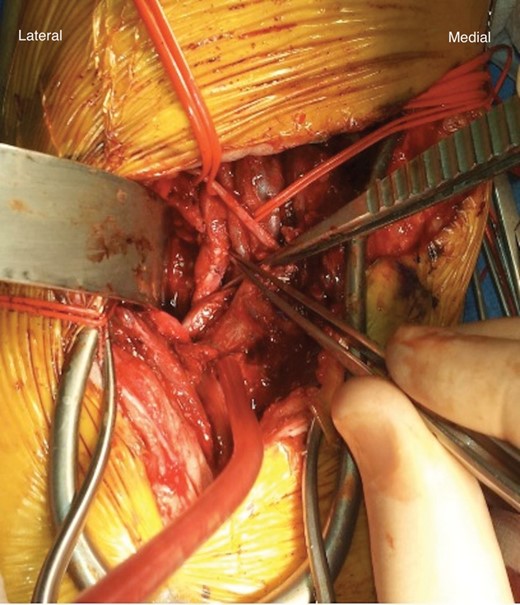
Venous patchplasty performed.
He was mobilizing well with a Zimmer frame on second postoperative day. He was discharged home within a week. At an outpatient visit after 2 weeks, his wound was well healed and he had good peripheral pulses.
DISCUSSION
Compartment syndrome in limbs occurs due to increased pressure within fascial compartments and inability of connective tissue to stretch. Common causes include long bone fractures, hemorrhage, ischemic reperfusion, burns, crush injuries, prolonged immobilization, substance abuse and carbon monoxide poisoning etc. [1–3]. Iatrogenic causes include knee arthroscopy, lithotomy position, improper use of elastic bandage and use of hypertonic saline [4–6].
In this case, the cause of compartment syndrome following arthroscopy can be 2-fold. One could be an accumulation of irrigation fluid passing through baker's cyst. Another more relevant factor could be iatrogenic popliteal pseudoaneurysm, causing compartment syndrome due to direct pressure effect.
The incidence of popliteal aneurysms is between 0.1 and 1%, while traumatic pseudoaneurysms constitute ∼0–3.5% of all popliteal aneurysms [7, 8]. The incidence of iatrogenic pseudoaneurysms is not reported yet in the literature. The iatrogenic popliteal pseudoaneurysm is caused by penetrating injury during any intervention around the knee joint, e.g. total knee replacement, arthroscopy of knee joint, acupuncture, femoral artery angiographic procedures, etc.
They may present with features characteristic of an aneurysm, e.g. pulsating mass, pain, nerve compression and rupture. Other presentations include thromboembolism causing limb ischemia, deep venous thrombosis and tumor [9]. In this case, it presented initially as compartment syndrome, and later investigations showed popliteal pseudoaneurysm to be the cause of this.
Diagnosis of iatrogenic popliteal aneurysm can be made with clinical examination and be confirmed with radiological investigations. Clinical examination may sometimes fail to reveal a pulsating mass due to significant swelling. However, if significant swelling appears following any knee intervention, iatrogenic pseudoaneurysm should always be suspected. An ultrasound should be performed as an initial screening tool, but investigation of choice would be a CT angiogram, that has sensitivity of 95.1% and specificity of 98.7% [10]. When compared with conventional angiogram, CT is quick, gives accurate results and is associated with less patient discomfort, and decreased cost.
Treatment modalities include ultrasound-guided thrombin injection, endovascular stent placement and open repair. Placement of endovascular stents is quick and less invasive, but is associated with deformation and failure. In this case, due to compression and displacement of the popliteal artery by pseudoaneurysm, open repair was performed. It resulted in a good outcome.
We suggest that a diagnosis of popliteal pseudoaneurysm should always be suspected, if significant calf/knee swelling appears following any knee intervention. An urgent ultrasound should be performed in such a scenario. A CT angiogram of lower limb not only provides dimensions of popliteal pseudoaneurysm, but also its pressure effects on adjacent popliteal artery. Open surgery appears to be successful treatment modality, when popliteal artery is found to be compressed and displaced.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}