





Abstract
Burkitt's lymphoma is an uncommon cause of intussusception in adults. Double intussusceptions due to Burkitt's lymphoma are extremely rare. We present a case of a 26-year-old man who presented with symptoms of intestinal obstruction and was diagnosed with double ileoileal intussusception at laparotomy. The pathology of the lead points turned out to be Burkitt's lymphoma. This could be the first reported case in the literature.
INTRODUCTION
Intussusception is rare in adults [1]. Intussusception was first described in 1674 by Barbette of Amsterdam and was given the name ‘introsusception’. The first successful operation on a child with intussusception was by Sir Jonathan Hutchinson in 1871 [2]. Unlike pediatric-type intussusception, adult intussusception harbors an organic lesion in 90% of cases [1]. Given the rarity of intussusception in adults, double intussusception is an even rarer condition [3]. We hereby present to you a case of double intussusception in a 26-year-old male patient due to intestinal Burkitt's lymphoma.
CASE REPORT
A 26-year-old male patient, previously healthy, presented to our ER complaining of diffuse colicky abdominal pain of one week duration. He also reported nausea, two episodes of non-bilious vomiting and a two-day history of constipation and obstipation. No fever or chills. He denied any past surgical history. His vital signs were all within normal limits. On physical examination, his abdomen was tender, distended and tympanic on percussion. Bowel sounds were hyperactive. DRE showed empty rectum. All his lab tests were normal except for mild leukocytosis. Plain abdominal film showed two air-fluid levels. A follow-up CT scan of the abdomen and pelvis showed small bowel obstruction and a 5 × 5 cm mesenteric mass (Fig. 1). Another mass of 3 × 3 cm was also noted. The patient was referred for surgical management.
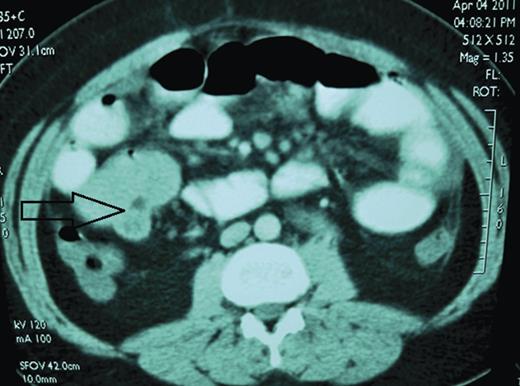
The 26-year-old man. Axial contrast-enhanced CT scan shows 5 × 5 cm small bowel mass (arrow). Operative findings confirmed ileoileal intussusception.
Under general anesthesia, patient in supine position, a midline laparotomy was performed. A large amount of abdominal fluid was aspirated and sent for culture and cytology. During running of the bowel at the level of 20 cm from the ligament of Treitz, an intussusception with a palpable intraluminal mass was found. Another intussusception 120 cm distal to the first was also noted (Fig. 2). No other pathologies were found. Double enterectomies with end-to-end anastamoses were performed. The patient was discharged home on Day 5 post op. Pathological analysis revealed polypoid and infiltrating intraluminal lymphoid proliferation (Fig. 3), extending to serosa and exhibiting diffuse aspect composed of medium-sized B-cells: pattern of Burkitt's Lymphoma. Abdominal fluid cytology analysis showed the presence of atypical lymphoid cells.

Intraoperative image of a double ileoileal intussusception. First one located ∼20 cm from the ligament of Treitz and the second about 120 cm distal to the first intussusception.
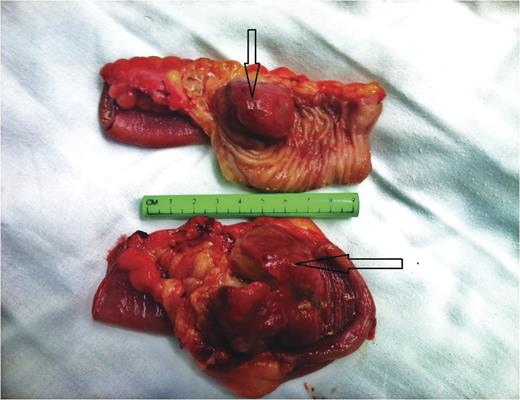
The surgical specimen comprised two segments of resected small bowel. Note the intraluminal mass (lead point) that caused the intussusception (arrows).
DISCUSSION
Intussusception is the invagination of a bowel loop with its mesenteric fold (intussusceptum) into the lumen of a contiguous portion of bowel (intussuscipien) as a result of peristalsis [4].
Intussusception is primarily a disease of infants and children with 90% showing no specific cause [1]. Adult intussusceptions represent only 5% of all intussusceptions [2, 4], causing 1% of intestinal obstructions, 0.003–0.02% of all hospital admissions [4] and 1/1300 of all abdominal operations [5]. Unlike in infancy, 70–90% of adult intussusceptions are due to some type of intestinal lesion [4]. Table 1 presents a comparison between pediatric and adult-type intussusceptions.
Comparison between adult and childhood intussusceptions [5]
| Adult | Childhood | |
|---|---|---|
| Incidence | Rare | 20 times as common |
| Mean age | 54.6 yrs | 2.2 yrs |
| m/f ratio | 1:1.3 | 3.6:1 |
| Idiopathic | 6.6–15% | 41% |
| Treatment | Surgical | Nonsurgical (67–90%) |
| Diagnostic yield | ||
| CT 52% | — | |
| Contrast 41% | 70% | |
| U/S 32% | 67% | |
Box 1 outlines some of the rare reported causes of intussusceptions [5].
Ca appendix
Adenomyoma in a Meckle's diverticulum
Submucous lipoma
Extramedullary haematopoeitic tumor
Haemangioma of small bowel
Endometriosis of terminal ileum
Peutz Jegher's polyp
Metastatic tesicular germ cell tumor
‘Vanished’ colonic tumor with deposits in glands
Pneumatosis coli
Coeliac disease
Ileal aberrant pancreas
Duodenal villous adenoma
Metastatic melanoma of ileum
Bowel wall haematoma
Gastroduodenal due to gastric carcinoma
Others
There are several proposed tools to aid in the diagnosis of intussusceptions. However, CT scan remains the most useful radiologic method for diagnosing intestinal intussusception according to several studies [2, 4]. Treatment of adult intussusceptions is usually surgical. Some advocate reduction of the intussusceptions, whereas others prefer resection without reduction, hence decreasing the likelihood of bowel injury or ischemia, and the dissemination or perforation of malignancy [1, 2, 4, 5]. However, Horton KM et al. found that intussusception is increasingly being detected by MDCT, even in asymptomatic patients, and given the recognition that intussusceptions may be transient, there is ongoing controversy regarding the optimal management, and have recommended that in asymptomatic patients, the CT identification of a proximal (jejunal), short (<3.5 cm) intussusception with a characteristic target sign and without obstructive symptoms may indicate a self-limiting process that can be managed conservatively. [6]. Double intussusception is extremely rare. There are four subtypes [3]:
Two separate intestines prolapsing into the same distal intestine, resulting in a characteristic ‘triple-circle’ sign on abdominal sonography and CT scan.
The double compound intussuception, which is extremely rare being reported once in the literature.
The double prolapse of the proximal and distal intestine through a patent vitello-intestinal duct.
Double-site intussusceptions, like the case we have presented.
Previous reports have shown that up to 50% of adult intussusceptions are due to intestinal neoplasms, including malignant lymphoma [4, 5].
The gastrointestinal tract is the most common extranodal site of lymphoma [7]; Pathologically, Burkitt's lymphoma and enteropathy-associated T-cell lymphoma, with MALT type are the most common lymphoma of the small intestine and account for 42.5% of the lymphomas [8]. Burkitt's lymphoma is a diffuse, undifferentiated, malignant monoclonal B-cell lymphoma with two major clinical presentations. American Burkitt's differs from the African type described by Burkitt in 1958 in its increased propensity for widespread involvement, especially within the abdominal cavity [9].
Surgery, chemotherapy, radiotherapy and radio-immunotherapy are the different modalities for the management of GI lymphoma and can be applied in different combinations [7]. Complete tumor resection with minimal complication is possible in most patients who present with intussusception, thus downgrading their stage of disease, hence requiring shorter duration and less intense chemotherapy minimizing the risk of early and late complications. [10].
According to the data from US SEER data for the period 1992–2005, the 5-year relative survival was 64.1% for lymphomas [8].
Hereby we presented to you a case of adult double intussusception due to Burkitt's lymphoma. There are many cases of intestinal lymphomas presenting with intussusception. To our knowledge, this is the first case of Burkitt's lymphoma presenting with intestinal obstruction due to simultaneous double intussusception to be reported.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}