





Abstract
Internal hernia is one of the rare causes of small bowel obstruction. A congenital mesenteric defect is very rare, but can potentially cause internal hernia with consequent incarceration or strangulation of the small intestine. An 18-year-old woman was brought to our emergency department with sudden onset lower abdominal pain. She had no remarkable past medical history and took no medications. An emergency laparotomy was performed. On exploring the abdominal cavity, the mesenteric defect was detected in the jejunal region, 3 cm in size. Loops of small intestine had gone through the defect three times in a complex manner and strangulated. Gangrenous intestine was resected and a primary anastomosis was performed. An adult congenital mesenteric defect is rare; however, it should be considered as one of the differential diagnoses in a relatively young patient with bowel obstruction without external hernia, previous abdominal surgery or trauma.
INTRODUCTION
Internal hernia due to congenital mesenteric defect has been reported in the field of pediatric surgery; however, adult cases have rarely been reported. Mesenteric defect can present with intestinal obstruction and cause incarceration or strangulation. We present a case of a previously healthy 18-year-old woman with congenital mesenteric defect that caused small bowel strangulation by an internal hernia.
CASE REPORT
An 18-year-old woman was brought to our emergency department with sudden onset lower abdominal pain. She had no remarkable past medical history and took no medications.
On physical examination, her abdomen was firm and an ∼15 cm fullness was palpable in the mid-to-lower abdomen, with severe tenderness.
Abdominal computed tomography (CT) revealed loops of edematous small intestines which possible gangrenous changes (Fig.1).

Computed tomographic scans of axial and coronal views of abdomen demonstrating edematous small intestines (arrows).
An emergency laparotomy was performed. On exploring the abdominal cavity, small intestine was necrotic. The mesenteric defect is detected in the jejunal region, 3 cm in size (Fig. 2). Loops of small intestine had gone through the defect three times in a complex manner and strangulated. The mesenterium needed to be incised to complete resection of necrotic small intestines. The gangrenous intestines were resected and a primary anastomosis was performed.
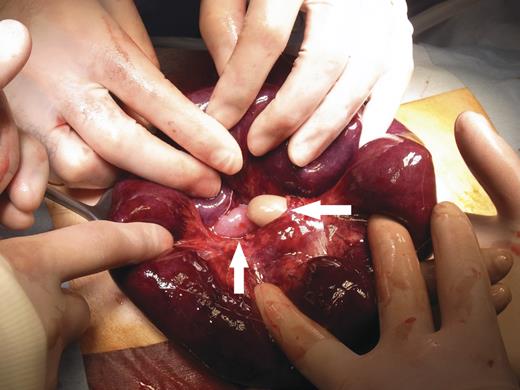
Intraoperative finding showing necrotic small intestines and a mesenteric defect (arrows) in the jejunal region.
The patient's postoperative course was uneventful and she was discharged on postoperative day 6 without any complications.
DISCUSSION
Internal hernia is one of the rare causes of small bowel obstruction. It is reported that 0.2–0.9% of patients of small bowel obstruction have internal hernia [1, 2]. A transmesenteric hernia is an unusual type of internal hernia. Transmesenteric hernia occurs more frequently after previous surgery in which mesenterium has been incised but not closed after gastro-intestinal reconstruction. On the other hand, a congenital mesenteric defect is very rare but can potentially cause internal hernia with consequent incarceration or strangulation of the small intestine. Congenital mesenteric defects causing internal hernia have been mostly reported in infants and children, and can become a cause of unexpected death. In adult patients, the causes of mesenteric defect are mostly traumatic or postoperative state.
Adult congenital mesenteric defect causing small bowel obstruction has been documented in only a few reports: five reports describing six patients in the past [1–5]. Only one patient was a man and six patients were women. The age of patients ranged from 18 to 38 years. It is reported that a congenital mesenteric defect more frequently identified in the distal ileum. The defect was found during surgical operation in six patients, and in the remaining one patient at the time of an autopsy after unexpected death.
In the present patient, the mesenteric defect is located in the jejunal region, 3 cm in size (Fig. 2). Her intestinal obstruction and strangulation were so complex that resection required incision of the mesenterium. Because she denied past abdominal trauma and had not undergone any previous abdominal surgeries, the mesenteric defect is considered as congenital.
The preoperative diagnosis of mesenteric defect is difficult because of wide range of acute abdominal symptoms, and there are no specific radiographic findings. It has been reported that CT can suggest the presence of internal hernia; however, there are no confirmatory findings for mesenteric defect [3]. The diagnosis has been made by surgery or autopsy. CT of the present patient suggested the presence of internal hernia but the cause of internal hernia was not determined. Emergency surgery was performed based not on CT findings but on clinical findings of highly suspected intestinal strangulation.
The causes of forming mesentery defect still remain uncertain. A few hypotheses have been reported, such as regression of the dorsal mesentery, developmental enlargement of a hypovascular area, the rapid lengthening of a segment of mesentery and compression of the mesentery by the colon during fetal mid-gut herniation into the yolk sac [6, 7]. It is also reported that congenital mesenteric defect is often associated with other anomalies of the gastro-intestinal tract, especially small bowel atresia. Malit et al. have suggested that isolated mesenteric defect represent a forme fruste (an atypical, especially a mild or incomplete, form) of intestinal atresia [7]. In the present patient, a small ectopic pancreatic tissue was found in the resected small intestine, and might be related to congenital nature of mesenteric defect. The location of most mesenteric defect is reported in the ileocecal (distal small intestinal) region, unlike in the present patient [1, 3].
Transmesenteric hernia is a rare cause of small bowel obstruction. A congenital mesenteric defect should be considered as one of the differential diagnoses in a relatively young patient with bowel obstruction without external hernia, previous abdominal surgery or trauma. Surgical decision-making is on the basis of clinical findings of intestinal strangulation or ischemia, and emergency laparotomy should be performed without preoperative diagnosis of such a rare disease. When mesenteric defect is incidentally detected during unrelated abdominal surgery, the defect should be closed to prevent it from causing internal hernia in future.

{kind=link}
{kind=link}
{kind=link}
{kind=link}