





Abstract
Herein, we report an unusual presentation of a 38-year-old heathy lady with a painless slowly growing lesion in the volar aspect of her left distal forearm reaching the thenar area for >15 years. Magnetic resonance imaging of the lesion showed multilobulated soft tissue mass with low and high signal in T1- and T2-weighted images with homogenous contrast enhancement. Additionally, a stable serpiginous bony lesion was noted in the first metacarpal bone showing low T1 and high T2 signals with peripheral enhancement. Histopathological examination was consistent with cylindroma and enchondroma, respectively. The patient had full recovery with no recurrence at a 1-year follow-up visit. While enchondroma is the most common benign tumor of the hand, sporadic dermal cylindroma, in contrast, rarely affects the upper extremity. The coexistence of these two pathological entities was not previously reported and it may complicate the diagnosis.
Introduction
Enchondroma is a benign lobulated bony neoplasm of hyaline cartilage origin [1]. It is the most common primary neoplasm of the hand [2]. Typically, they are slow-growing and can present with swelling, pain, deformity, fractures, or very frequently as incidental findings on X-ray [2]. While commonly present solitary, multiple enchondromas can occur (enchondromatosis) such as in Ollier disease and Maffucci syndrome [2]. No reports exist on the association solitary enchondroma with cylindroma.
Cylindroma is a benign adnexal neoplasia that can present as dome-shaped, smooth, solitary, or multiple nodular lesions predominantly affecting the head and neck [3]. Multiple scalp lesions resemble a hat hence the name “turban tumor” [4]. Middles-aged and elderly female are more likely to be affected [3]. The majority of cases are sporadic and present with solitary lesions affecting older individuals whereas patients with multiple lesions will most likely present at an earlier age and tend to be syndromic [3]. Herein, we present a rare case of forearm solitary cylindroma coexisting in close proximity to a solitary enchondroma of the first metacarpal bone.
Case report
A 38-year-old lady presented to our hand surgery clinic complaining of a left forearm swelling that initially appeared when she was a teenager as a small nodule with no proceeding trauma. The lesion then suddenly increased in size 13 years ago and kept growing slowly over the years. The lesion was only painful to touch; otherwise, she reported no history of skin changes, discharge, or sensorimotor deficits. Prior to presenting to our clinic, she was treated in another hospital with the presumptive diagnosis of vascular malformation for which she received two sessions of sclerotherapy with no notable improvement. Sclerotherapy was performed 15–20 years ago in different hospital since they suspected venous malformation. It is almost impossible to identify the agent since it was done long ago at a different hospital. Clinical examination revealed a firm multilobulated skin-colored non-mobile soft tissue lesion. Mild tenderness was noted upon examination. Vascular, motor, and sensory examination was unremarkable.
X-ray showed a well-defined non-aggressive lytic bony lesion of the first metacarpal bone (Fig. 1). Magnetic resonance imaging (MRI) showed a grossly stable skin and subcutaneous multilobulated soft tissue mass located at the palmar aspect of the wrist joint measuring 6 × 2 × 3.3 cm3 in its maximum anteroposterior, transverse and craniocaudal dimensions, respectively (Figs 2 and 3). The lesion showed low and high signals in T1 - and T2-weighted images with homogenous contrast enhancement. The lesion was inseparable from the flexor carpi radialis and palmaris longus tendons without definite invasion or encasement. The lesion was not in continuity, however, with the serpiginous lytic bony lesion noted at the first metacarpal bone exhibiting low T1 and high T2 signals with peripheral enhancement and no cortical destruction or associated soft tissue component (Fig. 4).
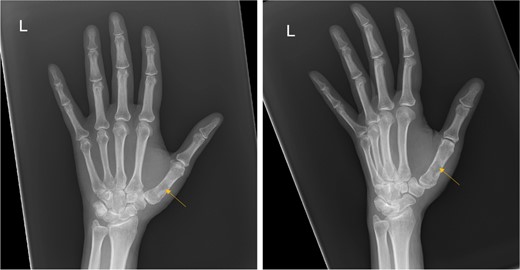
Frontal and oblique radiograph of the left hand showing a non-aggressive lytic lesion of the left 1st metacarpal bone with internal sclerosis.
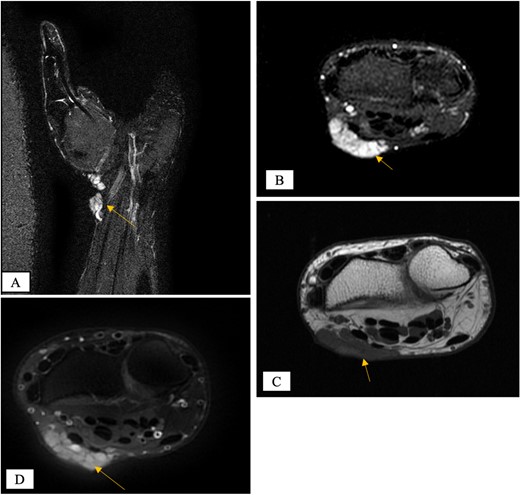
MRI of the left distal forearm showing cutaneous and subcutaneous lobulated mass at the volar aspect of high T2 and low T1 signals with diffuse enhancement. (A) Coronal T2-weighted fat saturated image. (B) Axial T2-weighted fat saturated image. (C) Axial T1-weighted image. (D) Axial T1-weighted fat saturated image post gadolinium injection.
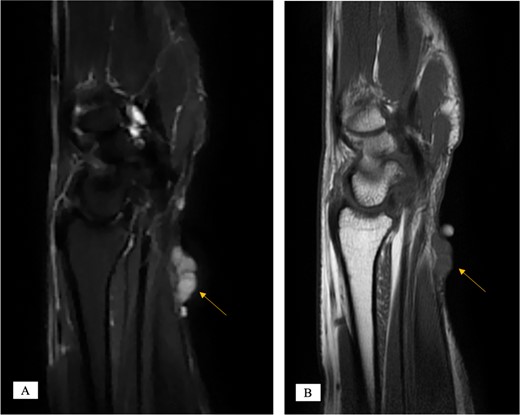
MRI of the left distal forearm showing cutaneous and subcutaneous lobulated mass at the volar aspect of high T2 and low T1 signals with diffuse enhancement. (A) Sagittal T2-weighted fat saturated image. (B) Sagittal T1-weighted image.
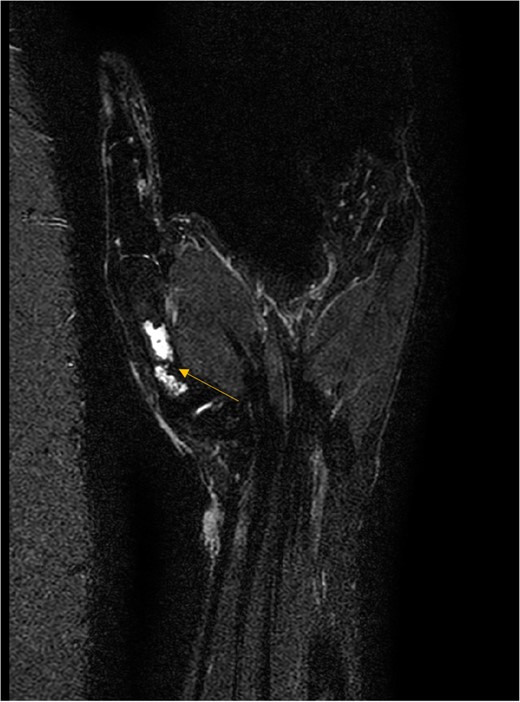
MRI coronal T2-weighted fat saturated image showing intraosseous lesion of high T2 signal in the first metacarpal bone.
Patient opted for surgical removal and excisional biopsy was done (Fig. 5). Histopathological examination revealed a nodular, well-circumscribed subepidermal proliferation of basophilic epithelial cells with “jigsaw puzzle” pattern and an eosinophilic stroma (Fig. 6A, B). No evident necrosis or atypical mitotic activity were identified. For further clarification, a panel of immunostains was performed (Fig. 6C, D). The immunostaining pattern of CD31, EMA, P63, and P16 highlighted the vascularized stroma and the epithelial components for the lesion along with a low Ki-67 proliferation index (1–3%). Therefore, the overall histological features and the well-circumscribed nodular proliferation were consistent with an eccrine cylindroma rather than vascular malformation or an atypical process. The lesion appeared to be completely excised with free surgical margins. As for the first metacarpal bone cyst, the patient opted for surgical removal despite the lack of aggressive or malignant feature. Intraoperative findings were in line with enchondroma. Curettage of the lesion and filling of the defect with bone substitute was performed. Histopathological assessment confirmed the diagnosis of enchondroma. The patient recovered well, without motor or sensory deficit, and no sign of recurrence at a 1-year follow up. Radiological follow-up of the hand showed good graft take with no recurrence.

Left distal forearm multi-lobulated soft tissue lesion.
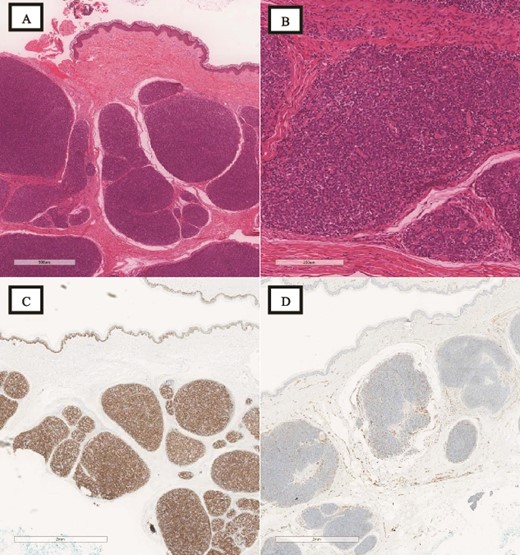
(A) H&E, low magnification (4×): the subepidermal proliferation of the basophilic epithelial cells appears to be organized in a “jigsaw puzzle” pattern rather than an irregular multinodular pattern. (B) H&E, high magnification (20×): although features with spiradenocylindroma are encountered, the dual cell population with thick intratumoral hyaline stroma and the “jigsaw puzzle” pattern, predominate mostly the Cylindroma component. (C) P63 immunostain: the solid pattern of the basaloid cells in the myoepithelial cell population is highlighted. (D) CD31 immunostain: the mostly peripheral vascular pattern of cylindroma rather than intratumoral vessels is highlighted. The overall tumor’s morphology has spiradenocylindroma features with a predominant cylindroma pattern.
Discussion
Cylindroma is relatively uncommon slow-growing benign adnexal tumor accounting for <1% of all adnexal tumors. The name cylindroma is derived from the histological appearance of the tumor when cut in cross section where the nests of cells have rounded cylinders-like morphology [4]. The pathogenesis of cylindroma has remained a subject of debate. While, conventionally, it is classified a tumor of apocrine origin due to their morphological resemblance of secretory cells, however; ultrastructural and immunohistochemical evidence has favored an eccrine origin [3, 5]. Moreover, those who are not in favor of eccrine differentiation account for the fact that cylindromas arise in the hair-follicle bearing areas of the skin rather than in palmar and planter surfaces that are rich in eccrine glands and devoid of pilosebaceous units and apocrine glands [3, 5]. The case that we report is not about the complexity of the case, it is more of reporting a rare pathology, which was initially wrongly diagnosed and managed. In the present paper, the lesion affected the volar aspect of the forearm with histopathological examination in support of eccrine differentiation.
Aside from the head and neck, sporadic cylindromas are not commonly diagnosed based on clinical examination and histological assessment is always needed for confirmative diagnosis. Microscopically, the lesion shows dual cell population; (i) peripherally-located undifferentiated compact basaloid cells and (ii) centralized differentiated polygonal-shaped cells with abundant amphophilc cytoplasm [3]. Both cell types have low mitotic activity, the nucleoli are usually inapparent with dispersed nuclear chromatin. Furthermore, cylindroma can be readily distinguished on low-power magnification by its cellular arrangement in a “jigsaw puzzle” fashion and deposition of eosinophilic hyaline material around the cellular nests in the dermal connective tissue [3].
Differential diagnosis of dermal cylindroma include spiroadenoma, a benign neoplasm of eccrine origin commonly affecting the head, neck, and trunk [6]. Although uncommon, it has been reported to affect the upper extremities [6]. On the other hand, sporadic cylindromas are very unlikely to present in the upper extremities with only one case reported in the literature [5]; Widayati et al. reported a diagnosis of the right arm dermal cylindroma presenting as two fragmented tan to white painless nodules affecting a 51-year-old lady.
In contrast, solitary enchondroma commonly affects the hand, and X-ray is the initial modality of imaging and might suffices for diagnosis; it appears as a well-defined lytic lesion [1, 2]. In more severe cases, thinning or disruption of the cortices can be seen for which osteosarcoma should always be included in the differential diagnosis [1]. Advanced images such as MRI might be needed based on individual cases to detail the tumor characteristics and surrounding soft tissue involvement and to help narrow the differential diagnosis [1]. In our case, MRI was utilized to further delineate the nature of the tumor and to assess for any connection if present with the soft tissue lesion present in proximity.
Treatment options for cylindroma include excision, laser ablation, and cryotherapy [3]. Excision is the preferred treatment and is usually curative. Large lesions should be imaged before planning treatment to determine the vascularity and involvement of surrounding tissues, including underlying osseous structures [3]. A recurrence rate of over 40% has been documented as well as the potential for malignant transformation [7]. Therefore, complete surgical removal with free resection margins and close follow-up is of great importance.
For enchondroma, controversy remains regarding the timing of surgical intervention and the filling modality for the resulting defect. Autogenous and allogenous bone graft, bone graft substitute, and a combination of thereof have been reported with good outcome. For symptomatic lesions, the standard of care is curettage [8]. Large lesions as well should be considered for surgical removal. In the present case, patient opted for surgical removal. Augmentation of the defect with bone substitute yielded optimal functional and radiological results without donor site morbidity.
Conclusion
Herein, we report an unusual presentation of non-syndromic dermal cylindroma and a solitary enchondroma. While enchondroma is a common pathology of the hand, sporadic cylindroma commonly affects the head and neck region and is rarely reported in the upper extremity. Besides the uncommon location, the coexistence of these pathological entities in the same anatomical region can further complicate the diagnosis. The knowledge of possibility of such presentation will broaden the armamentarium of hand surgeon. Thorough history, physical examination, and investigation are needed to narrow differential diagnoses and guide optimal treatment modality with least patient morbidity.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}