





Abstract
Acute appendicitis supposedly results from appendix obstruction caused by various conditions, including caecal cancer. Here, we report an adenocarcinoma found in the specimen of a 65-year-old man diagnosed with acute appendicitis. The adenocarcinoma was detected in the appendix stump after emergency laparoscopic appendectomy. The patient was diagnosed with caecal cancer based on post-operative lower endoscopy findings, and an additional laparoscopic right hemicolectomy was performed. Acute appendicitis can occur at any age and may require emergency surgery. It is a benign disease that can be cured entirely by appendectomy in most cases but may result from an underlying malignant disease in some cases, especially in patients >40 years of age. Thus, clinicians should consider the possibility of a malignancy while diagnosing and treating acute appendicitis.
Introduction
The lifetime incidence of acute appendicitis is 6%–9%, according to various reports [1–3], and acute appendicitis is one of the most common abdominal surgical emergencies. Although the underlying mechanism of appendicitis is unknown, it is initiated as appendix obstruction by fecalith or lymphoid hyperplasia and rarely by neoplasms [2, 4]. The incidence of appendicitis caused by caecal cancer (0.7%–0.85%) increases to 1.6%–24% in patients >55–65 years [5–7]. Acute appendicitis is classified as uncomplicated appendicitis (UA) and complicated appendicitis (CA), which are treated conservatively and through surgery, respectively [2, 7]. Interval appendectomy is indicated during abscess formation caused by CA [7]; however, the cause may be neoplastic [8]. Herein, we reported an adenocarcinoma found in the specimen of a patient who underwent laparoscopic appendectomy for acute appendicitis, with caecal cancer discovered postoperatively.
Case presentation
A 65-year-old healthy man presented to the emergency department with persistent lower abdominal pain and vomiting. He exhibited tenderness throughout the lower abdomen, centred on the right lower abdomen, and muscular guarding, with no findings in the upper abdomen. Blood test results showed increased inflammatory findings (white blood cell 17 290/μl, C-reactive protein 0.19 mg/dl), and computed-tomography (CT) showed swelling of the appendix, increased density of surrounding fat tissue, and swollen lymph nodes (Fig. 1). We suspected gangrenous appendicitis and immediately performed laparoscopic appendectomy under general anaesthesia, which revealed perforation at the root of the appendix, indicating localized peritonitis. We performed an appendectomy and intraperitoneal lavage. As the postoperative inflammatory reaction persisted, we continued an antibiotic treatment. The patient was discharged on the 10th postoperative day.
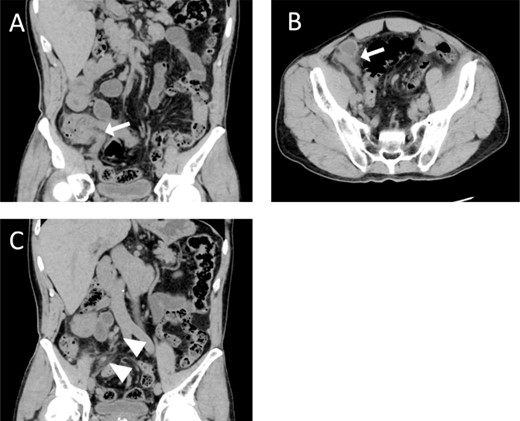
Computed tomography (CT) examination and postoperative pathological examination. Coronal (A) and horizontal (B) views show an enlarged appendix (white arrows). The coronal section (C) also shows enlarged regional lymph nodes (white arrowheads).
Pathological examination revealed adenocarcinoma at the surgical margin but not at the perforation site. We confirmed the intestinal tract findings seven weeks postoperatively using contrast-enhanced CT, revealing a contrast effect in the caecum and sustainably enlarged regional lymph nodes (Fig. 2A). A colonoscopy performed eight weeks postoperatively revealed advanced colon cancer in the caecum (Fig. 2B). The final diagnosis was acute appendicitis caused by caecal cancer-induced obstruction, requiring a right hemicolectomy with systematic lymphadenectomy performed nine weeks after the appendicitis surgery (Fig. 2C). The post-operative pathological diagnosis was T3N2M0, pStage IIIc (K-ras, wild type; BRAF, negative; MSI, low). Postoperative adjuvant therapy with capecitabine and oxaliplatin was initiated four weeks after the right hemicolectomy; no relapse occurred after ~10 months of chemotherapy.
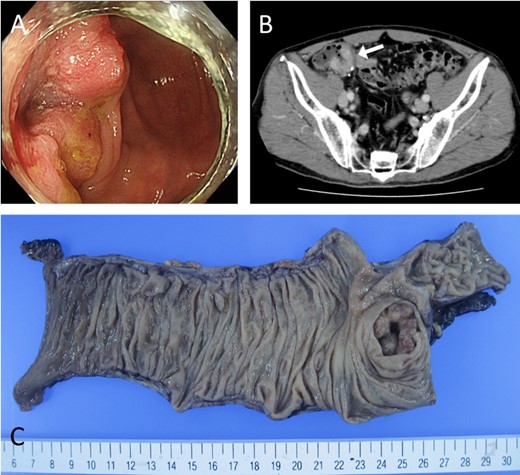
Preoperative evaluation for caecal cancer. (A) Colonoscopy reveals a type 2 lesion in the caecum with a central ulcer. (B) Contrast-enhanced CT shows that the tumour area was highly stained. (C) Macro-pathological examination reveals a type 2 lesion in the cecum.
Discussion
Appendicitis frequently requires surgical procedures; it has a lifetime risk of 8.6% (males) and 6.7% (females) in the United States [1]. Although the cause remains unknown [4], it may be caused by increased intraluminal pressure in the appendix due to obstruction, causing ischaemia of the appendiceal mucosa. The blockage prevents secretion, favouring bacterial overgrowth [2–4]. Obstructions are often caused by fecalith, lymphoid hyperplasia, or caecal neoplasia [2, 3, 5].
Appendicitis is broadly classified into UA without signs of gangrene or necrosis, and CA with gangrene, necrosis or perforation, and abscess formation [2]. The treatment strategies differ slightly, with appendectomy as the standard treatment [3]. Appendectomy for CA leads to a higher postoperative complication rate, requires a longer hospital stay, and may even require extended surgery, such as ileocecal resection, compared with that for UA [9]. Thus, the first choice for CA accompanied by an abdominal abscess and phlegm is conservative treatment using percutaneous drainage and appropriate antibiotics [7], despite its controversies. Patients with pneumoperitoneum or pan-peritonitis symptoms require emergency appendectomy [7]. In our patient, despite the absence of pan-peritonitis signs, abdominal pain was widespread in the lower abdomen, thereby necessitating emergency laparoscopic appendectomy to confirm the presence of perforation.
Appendiceal perforation is strongly age-related—being highest in older individuals and those aged <5 years—owing to diagnostic difficulties and less timely surgical interventions [1]. In older individuals, vascular sclerosis, lumen narrowing due to fibrosis, and fat infiltration into the muscle layer weaken the appendix tissue, making it more susceptible to perforation [7]. In our patient, the appendix was obstructed by a caecal tumour, resulting in perforation. There are two patterns of intestinal perforation due to malignant tumours of the gastrointestinal tract (especially colorectal): perforation in the tumour area (almost 70%) and proximal to the tumour site (~30%) [10]. The former increases the risk of peritoneal dissemination, although abdominal contamination is often localized, whereas perforation proximal to the tumour site may cause pan-peritonitis and septic shock due to diffuse faecal contamination [10]. Perforations caused by an appendiceal tumour can be divided into those in the tumour area and those in the dilated peripheral part of the appendix; the former ones have a worse prognosis [11]. In our case, a caecal tumour obstructed the appendix, causing dilatation and perforation in its distal part. Adjuvant chemotherapy was required because of observed regional lymph node metastasis.
In adults aged >55–65 years with acute appendicitis, the frequency of caecal or appendiceal cancer is 1.6%–24% [5, 7]. Among CA patients, especially those with an appendiceal mass due to inflammatory phlegmon or abscess, 10%–29% are at risk of a hidden malignancy in the colorectum [8]. Hence, colonoscopy screening is essential after an appendectomy, especially in patients with CA who undergo nonsurgical treatment [7]. A limitation of colonoscopy in acute appendicitis patients is the need for intestinal cleaning; pretreatment for active appendicitis may increase abdominal pain or cause complications, such as perforation or bleeding [12], for which the reported incidence is 0.038% [13]. To prevent aggravation or perforation, a colonoscopy is performed after the inflammation has subsided; this period is after 4–6 weeks for acute diverticulitis [14]. Such a waiting period may be necessary in acute appendicitis caused by appendiceal obstruction due to caecal cancer.
Our case highlighted that caecal lesions may be the underlying cause of the appendicitis, for which emergency surgery is commonly performed in daily medical practice. Therefore, when treating acute appendicitis in older persons, especially those aged >55 years, considering the possibility of a malignant tumour is necessary.
Author contributions
YN drafted the manuscript. YN, KT, and MY performed surgeries. MH supervised and approved the final version of this manuscript. All the authors have read and approved the final version of this manuscript.
Conflict of interest statement
The authors have no financial interest or financial support for the products or devices mentioned in this article. The authors declare no conflict of interest.
Funding
None declared.
Data availability
All data generated or analysed during this study are included in this published article.
Consent for publication
Written informed consent was obtained from the patient for the publication of this case report and the accompanying images.

{kind=link}
{kind=link}