





Abstract
Meckel’s diverticulitis is an unusual cause of acute abdomen condition in adults requiring prompt surgical treatment. We report a case of a 53-year-old male with coronavirus disease 19 (COVID-19), admitted to the emergency department with an acute abdominal pain. A computed tomography scan with intravenous contrast performed on the patient confirmed an inflamed short segment of the small bowel and the presence of a localized free peritoneal fluid. The definitive diagnosis was made intraoperatively, by means of an emergent ileal resection with primary anastomosis, which confirmed Meckel’s diverticulitis. Postoperative evolution was ordinary. The association of COVID-19 with the acute abdomen is found to be weak, therefore surgical consultation is advised to minimize delayed treatment.
INTRODUCTION
On March 2020, the World Health Organization declared a novel disease, caused by severe acute respiratory syndrome coronavirus 2, designated as coronavirus disease 19 (COVID-19). Symptoms are mainly respiratory manifestations and fever, but some patients may present mild abdominal symptoms [1]. Acute abdomen presentations are rare, and they occur mostly due to gastrointestinal ischemia. Therefore, abdominal imaging and surgical evaluation are required in these patients for differential diagnosis [2, 3]. Meckel’s diverticulum is the most prevalent congenital anomaly of the gastrointestinal tract, and its incidence rate of complications is approximately 4% in the affected population. Complicated Meckel’s diverticulum is less frequent in adulthood, and the most common presentation is intestinal obstruction followed by acute diverticulitis and bleeding [4, 5]. To our knowledge, this is the first report of a COVID-19 adult patient presenting a Meckel’s diverticulitis.
CASE REPORT
A 53-year-old man with a 10-day evolution of mild COVID-19 was admitted to the emergency department. He had a 2-day evolution, severe and sharp abdominal pain, which was located in the epigastrium, worsening in intensity on the last day. He also reported fever (38°C). The patient did not have nausea, vomit, abnormal bowel movements, other respiratory symptoms or urinary complaints. His medical history included arterial hypertension, dyslipidemia and a previous myocardial infarction submitted to coronary bypass surgery in 2013. A physical examination revealed a febrile (38.1°C) and stable patient (blood pressure (BP): 125/82 mmHg; hazard ratio (HR): 89 bpm). Cardiopulmonary auscultation was normal. His abdomen was non-distended, and tender mass in the epigastrium with localized guarding was noted. Bowel sounds were hypoactive and non-metallic. No abdominal hernias were identified. Laboratory exams revealed a normal white blood cell count (8.130/μl; segmented neutrophils, 72.9%), a hemoglobin level of 13.80 g/dl, a C-reactive protein level of 22.10 mg/dl, a d-dimer level of 0.94 μg/ml and normal hepatobiliopancreatic, cardiac and renal biochemical parameters. Urinalysis and the arterial-blood gas test were also normal. Ultrasonography was not performed due to its unavailability at the hospital on that day. A computed tomography (CT) scan with intravenous contrast of the abdomen was obtained, detecting a short segment of small bowel with inflammatory signs and localized free peritoneal fluid (Fig. 1). The pulmonary bases had residual ground-glass opacities related to COVID-19 (Fig. 2). Common diagnosis such as cholecystitis, pancreatitis or perforation of hollow viscus were ruled out. Given the lack of a preliminary diagnosis and the evidence of ongoing abdominal sepsis, the patient was proposed for a diagnostic and potentially therapeutic exploratory laparotomy. The intraoperative findings revealed a suppurative Meckel’s diverticulitis with local abscess, found at about 50 cm from the ileocecal valve (Fig. 3). Drainage and a segmental ileal resection with primary anastomosis were performed. In the postoperative period, inflammatory markers were responding positively to intravenous antibiotics and no further rises in temperature were observed. In addition, no complications were reported, and the patient was discharged on postoperative Day 6. The anatomopathological examination revealed small bowel with active inflammation and gangrenous Meckel’s diverticulum.
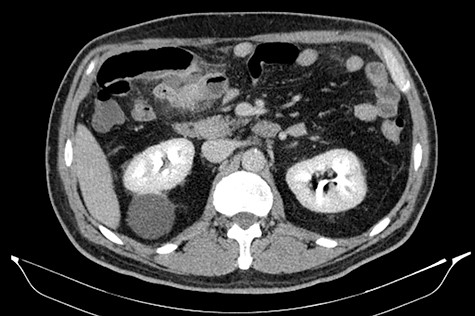
Short segment of small bowel with inflammatory signs and localized free peritoneal fluid (CT scan).
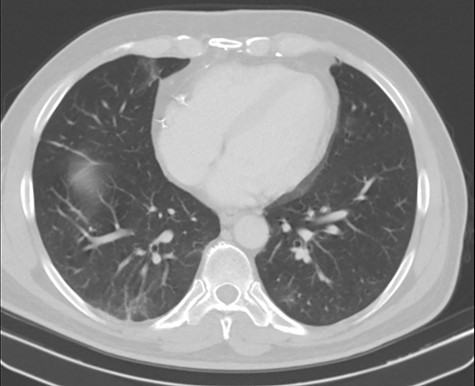
Residual ground-glass opacities related to COVID-19 (CT scan).

Intraoperative Meckel’s diverticulitis.
DISCUSSION
Despite being rare (2% of the general population), Meckel’s diverticulum is the most common congenital anomaly of the gastrointestinal tract, resulting from incomplete obliteration of the omphalomesenteric duct during the fetal life. Classically, it follows the 2’s rule: found in 2% of the population, twice more frequent in men, present before the age of 2 and located 2 feet proximal to the ileocaecal valve [4, 6]. In a large retrospective study with 1476 patients, the most frequent clinical presentations among symptomatic adult patients included bleeding (38%), intestinal obstruction (34%) and diverticulitis (28%) [7]. Diverticulitis usually occurs when diverticulum’s lumen has an obstruction resulting from a tumor or a foreign body or when ectopic gastric mucosa secretes acid within the diverticulum [8]. In the present case, none of the first postulated hypotheses was histologically confirmed. Diagnosis can be challenging as the clinical presentation and laboratory findings can mimic other abdominal diseases. Despite the accuracy of the CT scan being often low, the presence of a rounded or tubular collection of air and fluid that communicate with the small bowel and mesenteric inflammatory changes may suggest Meckel’s diverticulitis [4, 9]. Surgery is the standard of care, and surgical options include diverticulectomy or ileal resection in case of severe inflammation, perforation or tumor [7]. In the present case, an ileal resection with primary anastomosis was performed due to the inflammation of the ileum.
COVID-19 is a rapidly evolving disease and multiple studies concerning every aspect of the illness have added to the literature. For the purpose of emergency surgery, some features are worth noting. Some COVID-19 patients (especially those treated in the intensive care units may be at particular risk of developing complications such as bowel perforation or mesenteric ischemia. Furthermore, patients requiring emergent surgery may have concurrent COVID-19 infection, while postoperative patients can develop respiratory symptoms due to nosocomial COVID-19 infection. This requires the establishment of protocols to provide COVID-19 patients’ routes in the hospital and dedicated operating theaters and wards to prevent contamination of non-infected areas. Adequate personal protective equipment should also be available to limit the risks for health personnel [10]. Our hospital is a COVID-19-receiving hospital and since the outbreak in March, protocols have been implemented to provide COVID-19 patients with proper circuits. Ongoing studies postulate that COVID-19 may be associated with an increase of postoperative complications, but we report no complications in our patient. As far as we know, this is the first report of a COVID-19 adult patient presenting with Meckel’s diverticulitis. We also believe that SARS-CoV-2 did not play a role in the disease pathogeny, as no data are available in the literature to support such correlation.
CONCLUSION
Diverticulitis is one of the complications of Meckel’s diverticulum. Due to its rare manifestation in adults, preoperative diagnosis can be difficult, since its clinical, laboratory and imaging findings may overlap with other diseases. The treatment includes diverticulectomy or segmental resection. The COVID-19 pandemic brought new challenges to healthcare practitioners. Since the association of COVID-19 with the acute abdomen is weak, surgical consultation is advised to minimize misdiagnosis and avoid a delay in the treatment.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}