





Abstract
Surgical clip migration into the common bile duct (CBD) is a rare complication after laparoscopic cholecystectomy (LC). Few cases of surgical clip migration have been reported in the literature, and most of them have been successfully treated with endoscopic retrograde cholangiopancreatography (ERCP). We present a 71-year-old woman with 48 h of abdominal pain, jaundice and fever 6 years after laparoscopic cholecystectomy. She was diagnosed with common bile duct obstruction from surgical clip migration. After failure of ERCP, the patient was successfully treated with an innovative approach by laparoscopic transcystic extraction using endoscopic hose-type biopsy forceps. The presented technique was feasible and safe in expert hands, representing a valuable alternative to avoid the need of a choledochotomy in patients with unsuccessful ERCP.
INTRODUCTION
Surgical clip migration into the common bile duct (CBD) is a rare complication after laparoscopic cholecystectomy (LC) [1, 2]. Ligation of cystic artery and duct is usually performed with titanium surgical clips, which have the potential to migrate into the CBD with time and cause obstruction, stone formation, acute biliary pancreatitis, stenosis and cholangitis [2, 3]. Although most patients can be treated successfully with endoscopic retrograde cholangiopancreatography (ERCP), in up to 20% of patients this method fails, turning this case into true surgical challenges [2].
We herein report the case of a patient who experienced titanium clip migration into the CBD after LC and was successfully treated with an innovative technique of laparoscopic transcystic extraction after failure of ERCP.
CASE PRESENTATION
A 71-year-old woman with a history of LC for acute cholecystitis 6 years earlier was admitted with right upper quadrant abdominal pain, jaundice and fever. On admission, her vital signs were body temperature 38.2°C, pulse rate 96/min, respiration rate 21/min, blood pressure 100/60 mmHg and SpO2 98%. Her laboratory tests showed leukocytosis (19.200/ml), an erythrocyte sedimentation rate of 25 mm/h, C-reactive protein of 26 mg/l and altered liver function tests with cholestatic pattern: total bilirubin 4.95 mg/dl (normal up to 1.2), direct bilirubin 4.18 mg/dl, alkaline phosphatase 1083 IU/l (normal up to 150), gamma-glutamyl transferase 169 IU/l (normal up to 45), aspartate transaminase 281 IU/l (normal up to 40) and alanine transaminase 330 IU/l (normal up to 41). Serum amylase and lipase were normal. Abdominal ultrasound showed biliary tract dilatation but not obstructive cause, with a maximum diameter of the CBD of 17.6 mm. A subsequent magnetic resonance cholangiopancreatography (MRCP) found a filling defect in the distal CBD (Fig. 1). ERCP extraction was attempted, but it was impossible to progress the catheter due to an irregular distal bile duct stenosis. An abdominal computed tomography (CT) scan was therefore performed and showed a foreign body with radiopaque characteristics in the distal CBD consistent with a metallic clip (Fig. 2). Given that the object could not be removed by ERCP due to technical difficulties in biliary cannulation, laparoscopic bile duct exploration was decided.
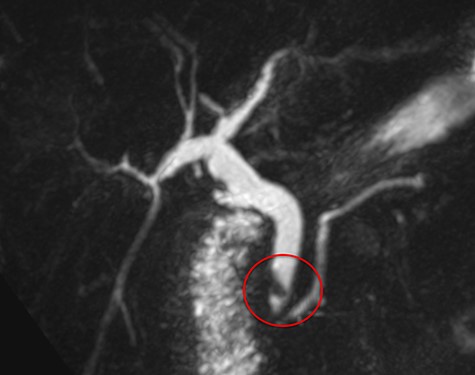
Magnetic resonance cholangiopancreatography (MRCP) showing a filling defect in the distal bile duct (red circle).
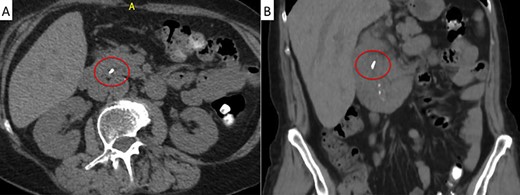
Abdominal CT scan. A metallic artifact is observed in the distal common bile duct (red circle) in axial (A) and coronal (B) planes.
With the patient in supine position, the trocars were placed as per the American technique of LC. After releasing lax adhesions, the remaining cystic duct was recognized and individualized from the CBD with cold scissors. Once isolated, a lateral incision in the cystic stump was made for CBD exploration (Fig. 3). Under radiological guidance, the clip was successfully removed through the cystic duct with endoscopic hose-type biopsy forceps (Fig. 4). A control cholangiography confirmed CBD clearance (Fig. 5). At the end of the procedure, the metallic clip was removed from the abdominal cavity (Fig. 6), and the remnant cystic stump was secured with a PDS Endoloop Ligature in order to avoid any future migration (Video 1 shows our technique). The patient recovered uneventfully and was discharged 3 days after surgery.
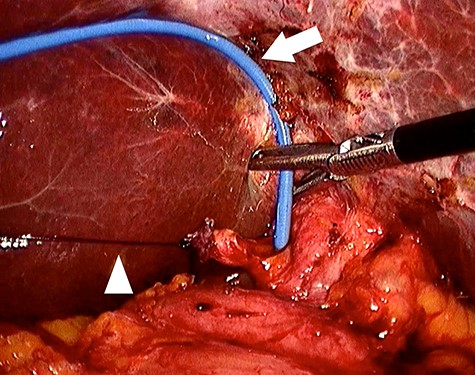
Four trocars were used, one in the umbilicus (12 mm), another in the epigastrium (5 mm) and two in the right hypochondrium (5 mm). An Endoloop ligature (arrowhead) is placed in the isolated cystic stump and exteriorized in the right hypochondrium for traction. This facilitates the incision in the cystic stump and the transcystic biliary exploration with endoscopic hose-type biopsy forceps (arrow).
DISCUSSION
We herein report for the first time a laparoscopic extraction of a migrated titanium clip into the CBD with an innovative transcystic approach using endoscopic hose-type biopsy forceps. After failed ERCP, this original alternative offered two very important advantages: first, the transcystic approach avoided the need of a choledochotomy, and second, the hose-type biopsy forceps allowed an easier catch of the metal clip compared with a Dormia wire basket. In addition, to the best of our knowledge, this is the first report to include a video describing in detail a laparoscopic CBD exploration to treat a migrated titanium clip after cholecystectomy.
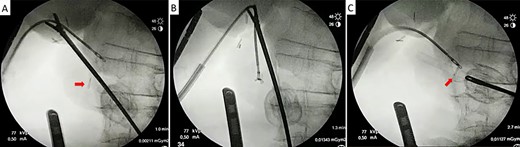
Laparoscopic transcystic extraction under intraoperative radiological guidance. Without any contrast injection to facilitate titanium visualization, the metallic clip (red arrow) is recognized in the distal CBD (A), caught with the endoscopic forceps (B) and finally removed from the CBD through the cystic duct (C).
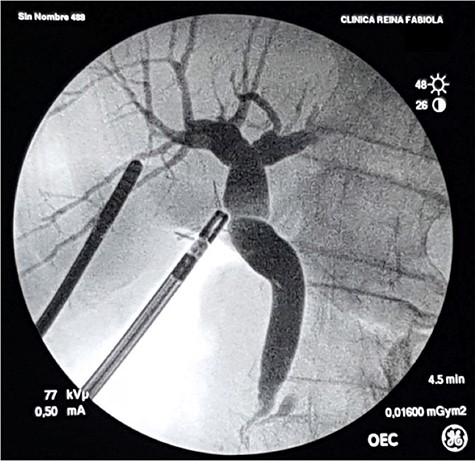
Control intraoperative cholangiography using a 5-Fr catheter and an Olsen clamp demonstrates free flow of contrast into the duodenum without defects or stenosis.
Although rare, metal surgical clips can migrate from their initial sites into the peritoneal cavity or adjacent structures such as the duodenum, venous vessels or bile ducts [1, 2, 4]. The first case was reported in 1979 after open cholecystectomy [5]. Later, Raoul et al. [6] reported a metallic clip in a large CBD stone after LC in 1992. The first case was successfully treated by laparotomy and the later by ERCP [5, 6]. Despite the large number of LC performed worldwide and the fact that metallic clips have become the most popular method of ligation, <100 cases of clip migration into the CBD have been reported [1, 2, 7]. Median time to clip migration has been reported to be 2 years, but it can vary from 11 days to 20 years [2]. The mechanism of clip migration is poorly understood and multiple hypotheses have been proposed [1, 2, 3–6]. One possible pathogenesis is the incomplete closure of the cyst duct due to ineffective clip placement, which leads to bile leakage or biloma and subsequent clip migration. Another pathogenesis could be the erosion of the bile duct wall due to localized chronic inflammation around the surgical clips. A short cystic duct, clip location near the CBD, suppurative complications, ductal wall ischemia due to excessive dissection and application of more than four clips have been reported as risk factors for this complication [1, 2]. Although other alternatives such as polymer locking ligation systems (Hem-o-lok) have been proposed, migration has also been documented with such devices [8]. In our opinion, as during the present case resolution, the cystic duct stump should be ligated with an absorbable suture material (PDS Endoloop) rather than with metallic clips. In the present case, a total of six clips were found on CT scan and laparoscopic exploration (two in the cystic duct, three adjacent to the CBD and one in the distal CBD). Therefore, it can be hypothesized that the three clips adjacent to the CBD may have been applied in a hurry to control bleeding and might inadvertently have pinched the CBD wall with its sharp edges. Progressive mechanic CBD wall erosion in the course of the healing process might have led to clip migration as proposed by other authors [9].

The metallic clip is recognized enclosed in biliary sludge. Notice that the clip is closed but both branches cross, denoting an incorrect closure.
Migrated surgical clips are foreign bodies that can act as a nidus for clip-related biliary stone formation [1, 2]. The clinical manifestations do not differ from those of ordinary choledocholithiasis, and ERCP is the treatment of choice, with a success rate of around 80% [2]. As in the present case, surgical treatment is reserved as a rescue procedure when ERCP fails [2]. In such scenario, the most common procedure is either open or laparoscopic choledochotomy with clip removal. Other minimally invasive therapeutic alternatives have also been described as rescue procedures, such as percutaneous transhepatic cholangiography with stone extraction and, to a much lesser extent, cholangioscopy [10–12]. In the present case, we propose an innovative laparoscopic approach including transcystic extraction with endoscopic hose-type biopsy forceps. Although the transcystic approach has many advantages and a success rate of about 87% among patients with choledocholithiasis [13], the limiting factors include anatomic features related to the cystic duct that hinder its cannulation and stone extraction, such as small size, tortuous duct, obstructive cystic valve, rupture of cystic duct during instrumentation in case of friable tissues and low level of insertion of cystic duct [14].
CONCLUSION
Surgical clip migration into the biliary tree is a rare complication after LC, and ERCP is the therapeutic procedure of choice. When ERCP is not possible or fails, other alternatives such as percutaneous or surgical exploration become mandatory. The presented technique of laparoscopic transcystic extraction was feasible and safe in expert hands, representing a valuable alternative which avoids the need of a choledochotomy.
CONFLICT OF INTEREST STATEMENT
None of the authors has any direct or indirect financial incentive associated with the publication of this manuscript, and all the funding involved in this work has been provided by our institution.
All the authors have made substantial contributions to this manuscript, participated in drafting the article and have read and approved the attached version.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}