





Abstract
Acute appendicitis is the most common surgical pathology worldwide, frequently, the patient history and clinical examination are so similar to other appendicular pathologies that preoperative diagnosis is almost impossible for the medical team. Neuroma of the appendix is a rare tumor of neural origin that usually resembles the symptoms of acute appendicitis. Pathology along with close follow-ups are key, as the diagnosis is based on the presence of nerve neuronal cells in the appendicular lumen. Surgical treatment is recommended due to the possibility of malignancy. We present a case of a 32-year-old male patient who presented with symptoms of acute abdomen, surgery was performed and appendectomy was completed. Neuroma of the appendix was the final diagnosis.
INTRODUCTION
Stromal tumors of the appendix include: leiomyoma, gastrointestinal stromal tumor and neurogenic lesions [1]. Neuroma of the appendix is a rare lesion on the appendix that is based on obliterative fibrosis co-occurring with hyperplasia of neural cells [1, 2]. Symptoms are non-specific and usually mimic acute appendicitis. Surgical treatment is recommended as this lesion is considered a precursor to carcinoid [2]. Histopathological examination is key as most patients are usually diagnosed as an incidental finding [1, 3]. We present a case of a young male patient who presented with symptoms of acute appendicitis and underwent surgery. After adequate treatment and close follow-up, he successfully recovered. Neuroma of the appendix was the final diagnosis.
CASE REPORT
Patient is a 32-year-old male without past medical history, he presented to the emergency room with a 5-day history of intermittent abdominal pain in his upper abdomen. At first, his pain was colicky and mild, nonetheless, as the days went by, the pain became much more severe and migrated to his lower right abdomen. On clinical examination, a febrile and dehydrated patient was encountered, his abdomen was very sensitive to gentle pressure and there was severe pain on sudden release of deep pressure in his lower right abdomen. Complementary exams revealed leukocytosis with neutrophilia and an elevated C reactive protein, computed tomography (CT) revealed slight inflammation of the surrounding retroperitoneal fat around the appendix (Fig. 1A and B). Acute abdomen due to appendicitis was suspected and surgery was decided. At surgery, on gross examination, the appendix measured 6 cm in length and 0.7 cm in diameter. The external surface of the appendix had a pink color with gray patches and showed congestion, no lymph nodes or other masses were found thus appendectomy was completed without complications.
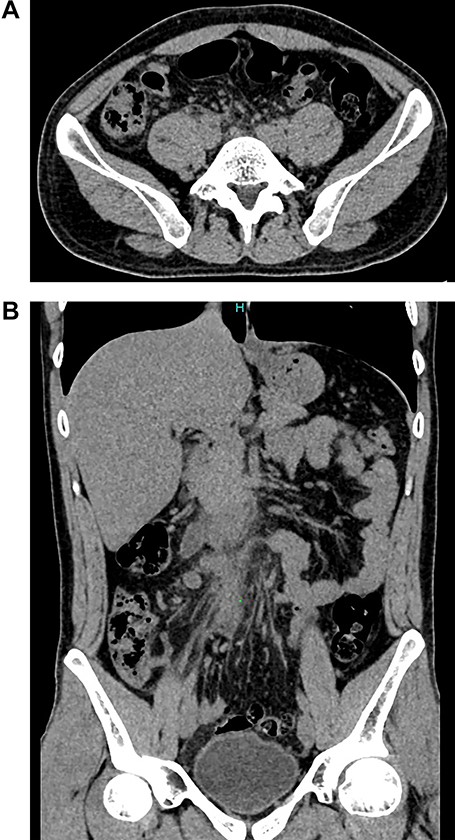
(A) CT, slight enhancement of the retroperitoneal fat. (B) CT, the appendix is seen with surrounded by retroperitoneum fat.
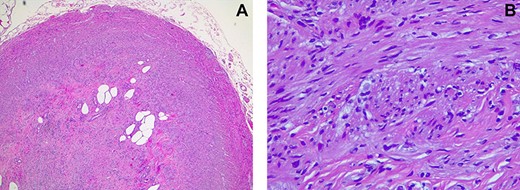
(A) Pathology, appendiceal lumen with complete obstruction due to proliferation of neural fusiform cells. (B) Pathology, neural fusiform cells without atypia.
Pathology revealed obstruction of the appendix and obliteration of its lumen by a proliferation of neural fusiform cells without atypia arranged in different directions accompanied by foci of mature adipocytes, they had immunoreactivity to S-100 protein and Neuron-specific enolase. Neuroma of the appendix was the final diagnosis (Fig. 2A and B).
His postoperative period was uneventful, diet was started on the first postoperative day and he was discharged soon after. On follow-ups, the patient is doing well.
DISCUSSION
Primary neuroma of the appendix is a rare tumor that was first described by the work of [1–3]. It was described as the proliferation of neural tissue that obstructs the appendiceal lumen causing fibrosis and obliteration of its lumen [2]. Although the physiopathology is not yet fully understood, it is believed that a persistent state of inflammation or repeated minimal subclinical attacks of inflammation within the appendix promotes the growth of neuroendocrine cells, non-myelinated nerves and Schwann cells that occlude the appendiceal lumen [1, 3]. Clinical manifestations are usually non-specific; however, in some cases it can be clinically indistinguishable from acute appendicitis [3, 4]. Patient anamnesis, symptoms, laboratory and physical examination can aid in the differential diagnosis. Nonetheless, most of these cases become evident only when the histopathology examination is available [1, 4]. In our case, the patient presented with an acute abdomen and surgery was decided. Pathology usually reveals an appendiceal lumen full of inflammatory cells and fibrous tissue, this tissue is accompanied by proliferating neuroendocrine and nerve cells, they can contain adipose tissue, fibrosis or eosinophilic infiltrate [1, 5]. Appendiceal neuromas show positivity for S-100 protein and neuron-specific enolase [1, 2, 5], as it was found in our patient.
Complete excision of the appendix is the treatment of choice, as appendiceal neuromas can be a potential precursor to malignant tumors since the enteroendocrine cells within the nerve bundles are hypertrophied and could be the origin of carcinoid [1–3]. The histology of the appendix shows a diverse perspective. Only in 0.1–4.2% of histopathologic evaluations abnormal diagnoses other than normal or inflammatory appendix are seen [6]. These rare diagnoses can potentially affect the patient’s management and prognosis [1, 7].
Pathology aid is an invaluable tool that only works if there is adequate follow-up. Health care providers must be fully aware of all these conditions that can only be diagnosed with a high commitment to the patient’s health and recovery. Close follow-ups are vital and an essential part of our work.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors declare that there was no funding.

{kind=link}
{kind=link}