





Abstract
Benign myofibroblastic lesions can clinically and histologically be mistaken for sarcoma. Excessive and potentially disfiguring surgical treatment can be avoided by ruling out malignancy. We present the case of a low-grade, myofibroblastic lesion of the lip, which shows how detailed clinical examination rather than reliance on histopathological information alone helped to achieve this. Differential diagnoses of myofibroblastic lesions are also discussed.
INTRODUCTION
Many lesions demonstrate a predominant myofibroblastic population. The more common of these are nodular fasciitis (NF), myofibroma, proliferative fasciitis, fibromatosis and myofibroblastic sarcoma. The first four lesions are benign but can exhibit histological features, which can be mistaken for malignancy [1–4]. It is therefore important that clinicians are aware of the distinctions between such lesions. We report a rare case of a benign, myofibroblastic lesion of the lip that histologically mimicked features of a sarcoma.
CASE REPORT
Two swellings had rapidly developed in the upper lip of a 17-year-old female, 3 months prior to presentation at the oral surgery department with a possible history of trauma. On examination there were two firms, smooth masses in the upper lip; one present in the midline and the other on the left side (Fig. 1) measuring 1 and 1.5 cm, respectively. The patient was asymptomatic with no history of pain or paraesthesia.
The results of ultrasound-guided aspiration were inconclusive with a report showing a scanty sample composed of bland spindle cells. The radiologist suggested provisional diagnoses of a peripheral nerve sheath tumour, NF or other spindle cell tumours and a core biopsy was recommended. Based on this information, an excisional biopsy of the larger lesion in the left side of the lip was undertaken (Fig. 2).
The samples showed fragments of a cellular tumour composed of fascicles of uniform myofibroblastic spindle cells set in a fibrous stroma (Fig. 3). The tumour exhibited infiltrative growth into skeletal muscle entrapping lobules of fat and small neurovascular bundles. Mitotic activity was 2/10 HPF and there was no necrosis, haemorrhage nor prominent blood vessels within the lesion. Immunohistochemistry showed that tumour cells were positive for smooth muscle actin (SMA) and calponin (Fig. 4). The samples were negative for H-caldesmon, CD34, S100, beta-catenin, desmin, myogenin and MyoD1. Studies have shown that the USP6 gene

Lesion of the upper left lip.
is a recurrent and specific finding in NF. However, molecular genetics showed that the USP6 gene rearrangement was not detected in this case. The histopathological opinion was that this was an infiltrative myofibroblastic tumour, which is difficult to classify. Molecular genetics and histopathological assessment stated that a low-grade, myofibroblastic sarcoma could not be excluded. Specialist soft tissue opinion was sought which corroborated the diagnosis.

Excisional biopsy of the lesion.
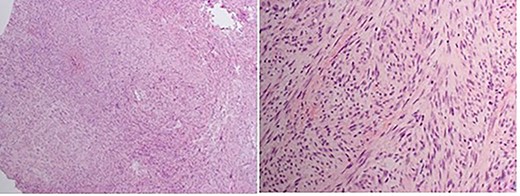
Haematoxylin and eosin stained section. Spindle cells arranged haphazardly and focally in poorly defined intersecting fascicles. Loose myxoid stroma with many vascular spaces in some parts. No cytological atypia or abnormal mitotic activity.
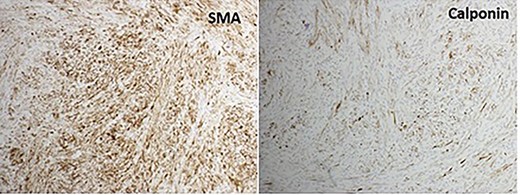
Immunohistochemistry for myofibroblasts. SMA and calponin stains the spindle cells.
The case was taken to a multidisciplinary team meeting where differential diagnoses and treatment options including surgery were discussed. Upon clinical review, however, the lesions reduced in size over the course of 1 month and were monitored with no further intervention required. With the clinical and histopathological information gathered, a probable diagnosis of NF was made.
DISCUSSION
Soft tissue pathology can be challenging due to the variety in morphology, rarity of certain types of soft tissue lesions and pathologists’ lack of experience of them [2]. Soft tissue pseudosarcomas are benign but their features of rapid growth, hypercellularity, cytologic atypia and mitotic activity can result in a misdiagnosis of sarcoma [1, 2]. In this case, a definitive histopathological diagnosis could not be ascertained but clinical presentation, imaging and histopathological features point to a diagnosis of NF. The most important lesion to consider in the differential diagnosis was soft tissue sarcoma [1–3]. Sarcomas can be differentiated as they lack myxomatous tissue found in NF. Sarcomas also show densely packed interweaving spindle cells, abnormal mitotic figures, necrosis and a marked degree of pleomorphism not found in NF. Sarcomas usually arise deeper in the soft tissue and are often larger and more infiltrative than NF. Another differential diagnosis includes fibromatosis but the negative stain for beta-catenin in this case excludes this. Myofibroma shows a frequent hemangiopericytoma (HPC)-like vascular pattern and biphasic pattern, which is lacking in NF. Proliferative fasciitis can be differentiated from NF since its characteristic ganglion-like myofibroblasts are absent in NF [4]. NF is rare but the most common soft tissue pseudosarcoma [2, 5] most often found in the upper extremities and trunk but rarely found in the orofacial region. Authors report an incidence of 7–20% of NF occurring in the head and neck region [5–10]. Many reports suggest that NF is reactionary to trauma [2–7]. Once excised, these lesions rarely recur but can also spontaneously regress which is why it is so important to exclude malignancy [1–10]. NF is most common in those aged between 30 and 50 years old [8] without a definite gender predilection (Figs 3 and 4) [10].
CONCLUSION
This case has highlighted the need for detailed clinical examination of patients and regular review, not only reliance on the histopathological diagnosis. The recommendation from histopathologists was to repeat excision. However, the clinical decision from the oral surgeons to monitor the lesions due to clinical features of regression meant that further aggressive treatment was not undertaken. It is essential that clinicians exclude malignancy in order to avoid unnecessary and invasive resective treatment for a benign lesion.
Conflict of interest statement
The authors have no conflict of interest to declare.
Funding
None.

{kind=link}
{kind=link}
{kind=link}
{kind=link}