





Abstract
Heterotopic pancreas is defined as pancreatic tissue found outside the usual anatomic location of the pancreas. It is often an incidental finding and can be found at various sites in the gastrointestinal tract. It is usually asymptomatic, however, symptoms such as abdominal pain, nausea, vomiting or even gastrointestinal bleeding could be possible.
In this report, a 38-year-old woman with epigastric fullness and endoscopic impression of the gastric submucosal tumor is described. Preoperative surveys including endoscopic ultrasound and computed tomography suggested gastric mesenchymal tumor such as leiomyoma. A surgical operation was arranged with a diagnosis of the heterotopic pancreas as confirmed by pathological assessment.
INTRODUCTION
Heterotopic pancreas is a rare anomaly. Although Schultz might have found this anomaly as early as 1729, however, Klob was the first to report such case with histology confirmation [1, 2]. By definition, heterotopic pancreas although without any vascular, neural or anatomical connection with the normal pancreas, exhibits at least one or all of the histological features of the pancreatic acinar formation. The most common presentation of the heterotopic pancreas is intraluminal submucosal protrusions with normal overlying mucosa [3]. This is the reason why they are usually diagnosed as submucosal tumors under routine endoscopy. The case presented today describes a lesion that is located at the posterior antrum of gastric with an initial impression of gastrointestinal stromal tumor (GIST) through endoscopic ultrasonography (EUS) and computed tomography (CT) examinations. Surgery was performed, and the final pathology diagnosis reported heterotopic pancreas in the stomach.
CASE REPORT
This is a 38-year-old female without any underline disease who came to our out-patient department due to a 2-month history of intermittent abdominal fullness and distension sensations. At first, she visited our gastroenterologist where medications promoting bowel motilities were prescribed but in vain. To further assess her condition, endoscopic ultrasonography was arranged which revealed a hypoechoic tumor with a diameter of 21.3 mm arising from the fourth layer of gastric wall. (Figs 1 and 2) An endoscopic biopsy was performed but reported negative findings due to failure in acquiring submucosal specimens on that biopsy. Based on epidemiology, gastrointestinal stromal tumor was suspected. Computed tomography was then arranged (Fig. 3) which revealed a submucosal tumor with heterogenous enhancement posterior wall of gastric antrum. No other lesion was found during that examination. Under such findings, she was then referred to a gastrointestinal surgeon for further surgical intervention.
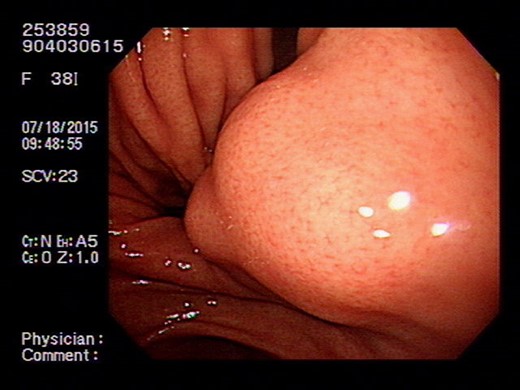
Endoscope showing intraluminal tumor with normal mucosal covering.
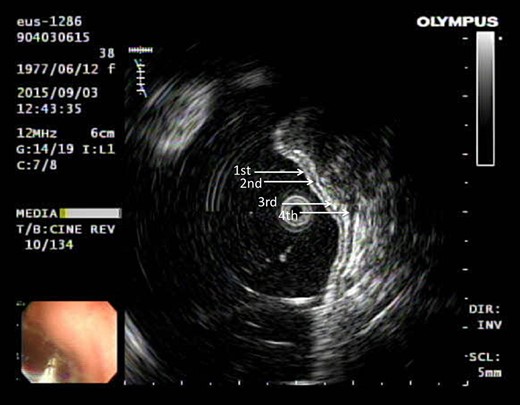
Ultrasonography showing tumor arising from the fourth layer of the gastric wall.
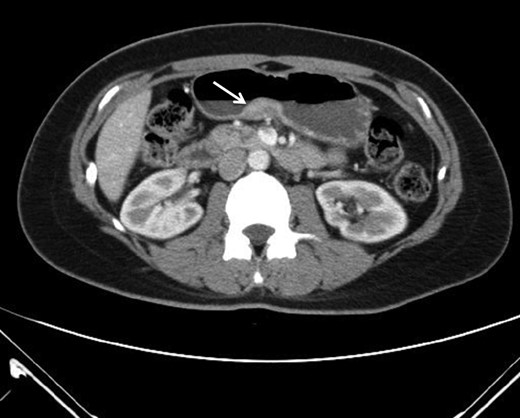
CT imaging revealing submucosal tumor at gastric antrum.
The operation arranged for this patient was laparoscopic partial gastrectomy. The size of the tumor excised showed a diameter of around 3 cm with intact mucosal layers and no gross extension over the serosa layer of gastric. Pathology report revealed heterotopic pancreas with microscopic features of pancreatic parenchyma lobules and dilated pancreatic ducts with involvements of muscle hyperplasia from submucosa to muscularis propria. No evidence of malignancy was shown and the patient was free from symptoms after the operation.
DISCUSSION
Heterotopic pancreas is a congenital anomaly with a reported prevalence of 0.5–13.7%. The most common locations are the upper gastrointestinal tract such as the stomach, duodenum and proximal jejunum. The less common sites are the esophagus, ileum and biliary tree. The diagnosis of heterotopic pancreas prior to surgery is difficult as it is generally asymptomatic. Besides, it also shares common features of the submucosal lesion under endoscopic (Fig. 4) or computed tomography examination. Although so, pathological changes similar to that of a normal pancreas (acute or chronic pancreatitis, cystic degeneration, malignant changes) are possible [4, 5]. Other than that, symptoms due to its anatomical position or tenderness resulting from the secretion of hormones and enzymes could all necessitate surgical interventions. By reviewing works of literature, we are able to gather some clues which might help us differentiate HP from other lesions before a treatment strategy is modulated. On conservative evaluations, a study conducted by Li et al. suggested that for masses <3 cm, a long diameter to short diameter ratio (LD/SD) greater than 1.29, enhancement value of >27.50 HU, enhancement ratio to pancreas of >0.72 are critical features [6]. Besides that, another study by Maryam et al. describes the MR imaging appearance of heterotopic pancreas mimics orthotopic pancreas. Characteristics of high signal intensity of the pancreas at T1-weighted imaging is useful for differentiation. Other than that, T2-weighted and MR cholangiopancreatographic images could help identify rudimentary or dilated ducts in the heterotopic pancreas to aid in differentiations [7]. Although endoscopic findings of central dimpling or umbilication which corresponds to an opening of a duct are the typical endoscopic finding for heterotopic pancreas, Haetaek et al. reported that it is seen in only 1/3 of cases. However, by using magnifying endoscopy with narrow band imaging, they can identify microscopic opening in more than 80% of lesions without a macroscopic opening, which suggests the possible usefulness of this method in predicting the diagnosis of heterotopic pancreas [8]. As for intervention approaches, endoscopic ultrasonographic fine needle aspiration (EUS-FNA) was reported to have a high sensitivity but somewhat limited diagnostic accuracy due to the limited quantity of tissue sample. A new technique of incorporating endoscopic submucosal dissection known as submucosal endoscopy with mucosal flap (SEMF) which could directly visualize the tumor or perform core biopsies has reported specific features of heterotopic pancreas as ‘yellow, cloudy, and soft with small nodule appearance similar to the pancreas.’ This endoscopic visualized features (EVF) could provide clues for the diagnosis of heterotopic pancreas. If uncertain, this technique could also provide the convenience of core biopsy samples for diagnosis prior to surgeries [3].
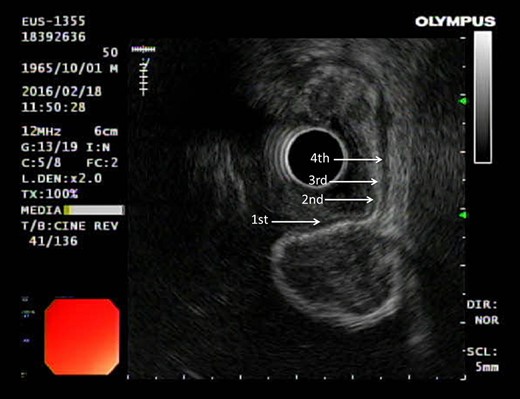
Gastrointestinal stromal tumor (GIST) under ultrasonography also shares similar feature by arising from the fourth layer of the gastric wall.
CONCLUSION
Although being rare, heterotopic pancreas should always be included as a differential diagnosis when assessing a submucosal tumor of gastrointestinal tract because failure to do so could lead to misleading and unnecessary excision. This paper revised some reported methods which could help us reach a more accurate diagnosis for treatment planning. However, due to the quality or sample size of the studies, further evidence might be needed to confirm the validity of the methods.
CONFLICT OF INTEREST STATEMENT
None.

{kind=link}
{kind=link}
{kind=link}
{kind=link}