





Abstract
It is estimated that up to 25 000 UK residents are exposed to small amounts of carbon monoxide (CO) annually. Symptoms of chronic exposure to CO are vague and non-specific and include dizziness and hearing loss. We describe a case of 38-year-old lady presenting with a 4-month history of vertigo and hearing loss. Initially diagnosed as Meniere’s disease, the patient was investigated and followed up in the clinic. She reported leakage of carbon monoxide from her gas fire identified during a routine safety check. Her symptoms fully resolved after disconnecting the faulty gas fire. A rare cause of fluctuating hearing loss and vertigo is described, and the diagnostic challenges are discussed.
INTRODUCTION
Carbon monoxide (CO) is odourless and colourless gas, often found in houses secondary to incomplete combustion of fuels. Accidental CO poisoning remains under-diagnosed as the source of CO is often not obvious and may be remote. Also, the symptoms of poisoning are often non-specific, further delaying diagnosis [1]. It is estimated that up to 25 000 UK residents are exposed to small amounts of CO annually [2]. Symptoms of chronic exposure to CO include impaired concentration, sleep disturbance, emotional lability, fatigue, dizziness and hearing loss [3]. The most common source of CO poisoning in domestic setting is a faulty heating system [1]. Lumio [3] first reported chronic CO poisoning in Finland in 1948, describing hearing loss and vertigo. Lakhani and Bleach [4] also reported isolated symptom of dizziness in a patient from chronic CO exposure from a faulty domestic boiler. We report a case of subacute CO poisoning, presenting with unilateral low frequency hearing loss and vertigo. The patient’s symptoms fully recovered once the source of CO was removed.
CASE REPORT
A 38-year-old Caucasian lady living alone in a bungalow, presented to the ENT out-patient clinic with a 4-month history of vertigo and hearing loss. She described her symptoms as episodes of light-headedness amounting to vertigo and lasting up to half an hour on each occasion, several times per day. There was no associated nausea or vomiting. She reported intermittent hearing loss, mainly on the right side but denied the presence of tinnitus. She also suffered with heaviness and pressure sensation in the head. There was no postural variation to her symptoms.
Examinations of her ears were normal but pure tone audiogram revealed right sided mild low frequency sensorineural hearing loss. Hearing thresholds were elevated at 30–40 dB in the right ear (Fig. 1). Hearing in the left ear was within the normal range. There was no nystagmus. She had normal gait, with normal Romberg’s and Unterberger’s tests.
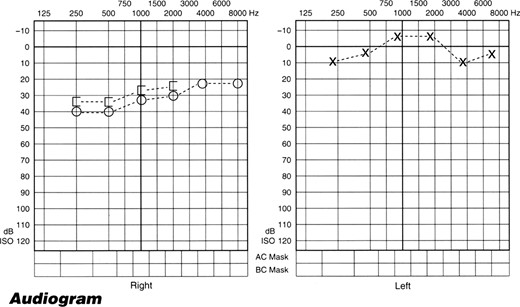
Pure tone audiogram showing 30–40 dB sensorineural hearing loss in the right ear mainly affecting the low frequencies.
Haematological and biochemical tests including thyroid function tests were normal. MRI scan of brain and internal auditory meatus revealed no abnormality.
The presence of episodic vertigo and fluctuating low frequency hearing loss, raised the possibility of Meniere’s disease. She was commenced on regular betahistine 16 mg three times a day. The patient returned after 3 months for a review and informed no noticeable change in her symptoms. Pure tone audiogram revealed an improvement and the bone conduction thresholds in the right ear were 25–30 dB. The left ear hearing remained normal. A neurologist’s consultation was requested and reported as normal.
The patient was further reviewed in the clinic four months later with complete resolution of her symptoms. Her hearing tests showed normal threshold in both ears (Fig. 2). She reported that a leakage of CO was identified from her gas fire during a routine annual safety check up. Since she had the gas fire disconnected, her symptoms resolved completely. A further review after 12 months confirmed no recurrence of symptoms and normal hearing thresholds.
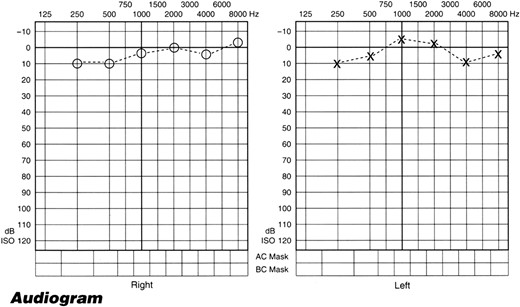
Pure tone audiogram showing hearing levels return to normal in the right side.
DISCUSSION
Lumio documented 78% incidence of SNHL among 700 cases of chronic CO poisoning [3]. CO functions as a neurotransmitter in physiological amounts, however, as the duration and the level of exposure increases CO produces toxicity, the exact mechanism of which is not fully understood [5, 6]. Pathophysiological explanations of the hearing loss following CO exposure are varied. Previous literature explains association of CO poisoning and hearing loss due to damage to cochlea, vestibular nerve and central auditory pathways [7].
Auditory dysfunction caused by CO appears to be frequency specific and basal region (high frequency) of cochlea appears to be selectively vulnerable to CO [8]. The CO-induced hearing loss is usually bilateral, with variable severity and affecting mostly high frequencies, but further exposure to CO may affect low frequencies as well [7]. Although rare, unilateral hearing loss due to CO poisoning has also been previously reported [9]. Our case report differs as it demonstrates a reversible low frequency SNHL due to CO poisoning not previously reported in literature. The association of reversible sensorineural hearing loss with subacute or chronic CO poisoning is not clear [1]. Our report highlights the possibility of other unknown mechanisms through which CO induces damage to cochlea. Our patient showed complete resolution of symptoms after removal of CO source without any specific treatment, suggesting recovery can be spontaneous and complete in mild CO-induced SNHL after removal of CO source.
In unexplained causes of SNHL, CO poisoning should be considered as a diagnostic possibility especially in ENT out patients settings. This is supported by the fact that missed diagnosis of CO intoxication can occur easily, as commonest symptoms are non-specific. Inexpensive and non-invasive tests such as CarboxyHaemoglobin (CoHb) measurements should be considered when investigating for unexplained hearing loss, especially in combination with other symptoms [10]. In our patient we were unable to check CoHb as the diagnosis was made retrospectively. Early recognition of this phenomenon and subsequent management may reduce the morbidity and improve recovery from any consequent hearing loss.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}