





Abstract
Diagnosing acute abdominal pain will always be a challenging task, patients frequently present with atypical symptoms. It is crucial for a clinician to have good differential diagnosis to avoid delay in diagnosis and treatment. We present 37-year-old male who presented to emergency department with 2 days of abdominal pain. The pain started centrally around his umbilicus and localized to his right upper quadrant (RUQ). Clinical examination showed he has localized peritonitism on the RUQ hence he was further investigated with CT abdomen. CT revealed he has appendicitis. This is due to the congenital anomaly where he has congenital agenesis of his right kidney. This case illustrates in patients with congenital agenesis of right kidney, the diagnosis of acute appendicitis should be considered in right upper quadrant pain. He was commenced on IV antibiotics and proceeded to have laparoscopic appendicectomy. He had an uneventful post-operative recovery.
INTRODUCTION
Acute appendicitis is a common pathology and often difficult to diagnose due to various atypical symptoms. It can also present with in atypical location and could be easily missed. Delayed diagnosis of acute appendicitis may increase the complication rate of appendicitis. It is often due to malrotation of the caecum resulting in non-descend of the caecum thus having a subhepatic appendix location.
CASE REPORT
A 37-year-old male presented to Emergency Department with 2 days of abdominal pain. The pain was initially peri-umbilical but localized to right upper quadrant on the day of presentation. He was also complaining of anorexia. He was febrile in the emergency department. Initially workup performed by Emergency Physicians showed he had white cell count of 6.60 × 109/L and raised CRP of 28. He was referred as acute cholecystitis to the General Surgeons in the hospital.
Upon review and clinically examination, the possibility of atypical appendicitis was raised due to the clinical history. Patient did not have any history of biliary colic or any epigastric pain. He was further investigated with CT abdomen which revealed the diagnosis of acute appendicitis in the right upper quadrant (Fig. 1). The atypical position of his presentation was a result of congenital right renal agenesis (Fig. 2). The appendix was lying on the right upper quadrant due to the absence of right kidney. He also had left kidney hydronephrosis and hypertrophy.
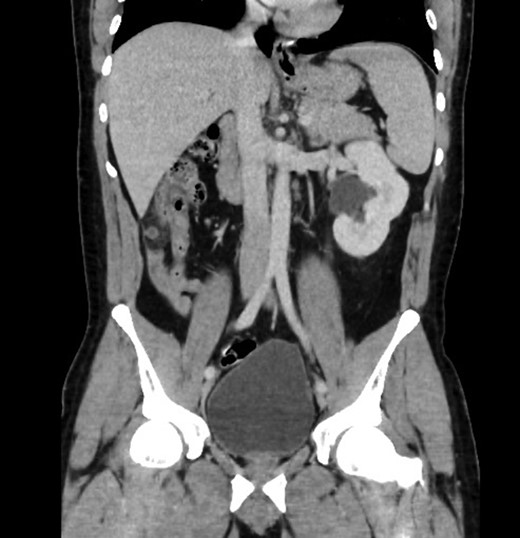
Sagittal view showing mal-descend of caecum secondary of congenital agenesis of right kidney, this resulted in subhepatic appendicitis.
He was referred on for emergency laparoscopic appendicectomy. This was performed with routine approach via three ports (Hasson’s technique entry umbilical, 2 × 5 mm port to the suprapubic and left iliac fossa). He recovered well and was discharged. The histopathology of the appendix confirmed acute appendicitis.

Axial view showing absence of right kidney due to congenital agenesis. Appendicitis with faecolith.
DISCUSSION
Acute appendicitis accounts for 1% of surgical operations. Various atypical appendix position have been described which includes retrocaecal (65.28%), pelvic (31%), subcaecal (2.26%), preileal (1%) and postileal (0.4%) [4]. Subhepatic appendix have been described due to maldescent of caecum [2, 3]. This case is unique as the congenital anomaly causing the subhepatic appendix is due to congenital agenesis of the right kidney. This has resulted a different clinical presentation which caused the pain to localized to the right upper quadrant instead of right lower quadrant. This will mislead most clinicians and delay the diagnosis subsequently treatment. The first described subhepatic appendix by King [1]. This is often misdiagnosed as acute cholecystitis. Abdominal ultrasound might be helpful but most often will show a normal gallbladder with traces of free fluid [2, 3].
Acute appendicitis in the right upper quadrant can mimic other diagnosis and will be a diagnostic dilemma. CT abdomen will provide more information if the clinical history suggests atypical symptoms for biliary pathology. This will reduce the delay in treatment and prevention of perforated appendicitis.
CONFLICT OF INTEREST STATEMENT
The authors have no commercial associations that might be a conflict of interest in relation to this article.
CONSENT
Consent has been obtained patient for this case report.

{kind=link}
{kind=link}