





Abstract
A large lingual cyst was noted on the 22-week antenatal ultrasound, which grew in proportion to the foetus on serial imaging. An elective c-section was performed in view of possible airway obstruction, and the neonate initially required oxygen to maintain saturations. Aged 1 month, the baby developed significant breastfeeding difficulties secondary to rapid cyst and secondary tongue enlargement, completely filling the oral cavity. Fifteen millilitres of fluid were aspirated in clinic, resulting in reduction of tongue size and immediate improvement in feeding. The patient subsequently underwent surgical excision of the cyst, which filled most of the anterior two-thirds of the tongue up to the foramen caecum. Histology supported the diagnosis of lingual thyroglossal duct cyst. A rare variant of thyroglossal duct cysts, these cysts can be potentially difficult to manage. More commonly located in the tongue base, we present an even rarer variant, that of an anterior tongue cyst.
INTRODUCTION
We describe a rare case of a baby with a lingual thyroglossal duct cyst, detected antenatally. Lingual thyroglossal duct cysts (TGDC) are important to detect as they can cause airway obstruction and respiratory distress as well as feeding difficulty. This case is even more interesting as lingual TGDC are normally found in the tongue base, whereas in this baby the cyst was located anteriorly.
CASE REPORT
A foetus was noted on the 22-week scan to have a large intralingual mass posterior to the foetal lips. It was deemed to be fluid-filled and measuring 19.6 mm × 16.8 mm × 24 mm. The mother was therefore referred to a tertiary foetal medicine department to be reviewed. Serial ultrasound and MRI imaging showed that this defect grew in proportion to the foetus (Fig. 1a and b). In view of concerns of potential airway obstruction at birth, an elective caesarean section was performed at 39 weeks gestation, with paediatric and otolaryngology teams present. At delivery, a large anterior tongue filling the oral cavity was noted, and the neonate initially required oxygen to maintain saturations. The baby was admitted to Neonatal Intensive Care Unit for observation, and was initially started on nasogastric feeds while assessing the effect of the oral cyst on the neonate’s ability to feed. The baby improved, maintained its saturations on air and it was found that the cyst did not impair oral feeding. The baby was therefore discharged from hospital at age 2 days with planned paediatric otolaryngology follow-up.
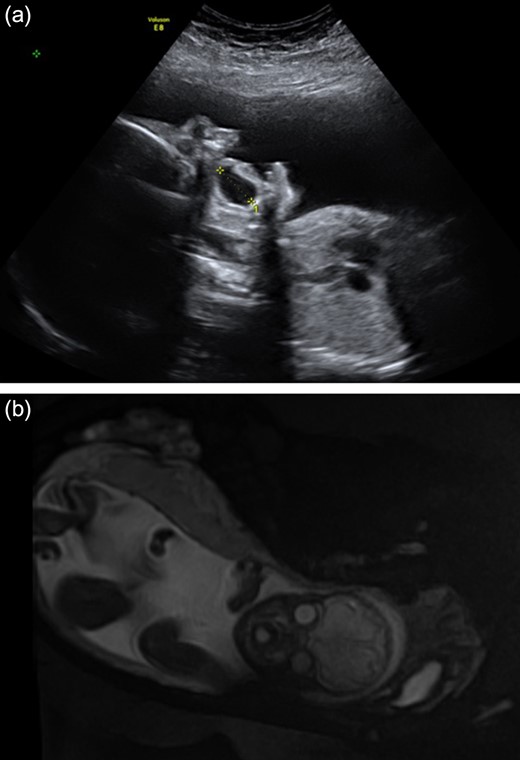
(a) and (b) Antenatal ultrasound at 28 weeks and MRI scan at 31 weeks demonstrating large fluid-filled oral cyst.
Clinic follow-up was expedited at age 5 weeks, as the cyst had increased rapidly in the preceding 10 days, resulting in impaired feeding. On examination, there was considerable swelling of the anterior tongue and floor of mouth, and the tongue was pushed superiorly against the hard palate and anteriorly, protruding past the lips. Interestingly there was no airway compromise. Fifteen millilitres of grey-brown fluid were aspirated from the cyst, which provided immediate reduction in swelling and improvement in feeding. It was planned to review the baby in 3 weeks with a view to future surgical excision, but to await microscopy and culture of the fluid and allow the neonate to grow further. Culture of the fluid showed no bacterial growth. However, at follow-up the cyst had re-collected to fill the entire oral cavity. Again there were no signs of airway compromise. Twenty millilitres of fluid were aspirated and the patient was booked for urgent surgical excision of the cyst. A horizontal sublingual incision above the submandibular duct openings was performed. The submandibular ducts and lingual nerves were identified and preserved. A cyst measuring 48 mm × 20 mm × 5 mm was excised, which extended up to the foramen caecum posteriorly (Figs 2–4). The defect was closed with vicryl rapide 4/0, and a small opening was left anteriorly and posteriorly to facillitate drainage. Histology showed that the cyst wall was lined by stratified squamous epithelium in some areas and bundles of smooth muscle in others. Additionally, there were small cystic structures lined by mucin-producing columnar cells. These appearances were consistent with the clinical diagnosis of a cystic thyroglossal duct remnant.

Pre-operative photograph of superior aspect of tongue demonstrating significant tongue swelling, resulting in the tongue protruding past the lips.

Pre-operative photograph of inferior aspect of tongue.
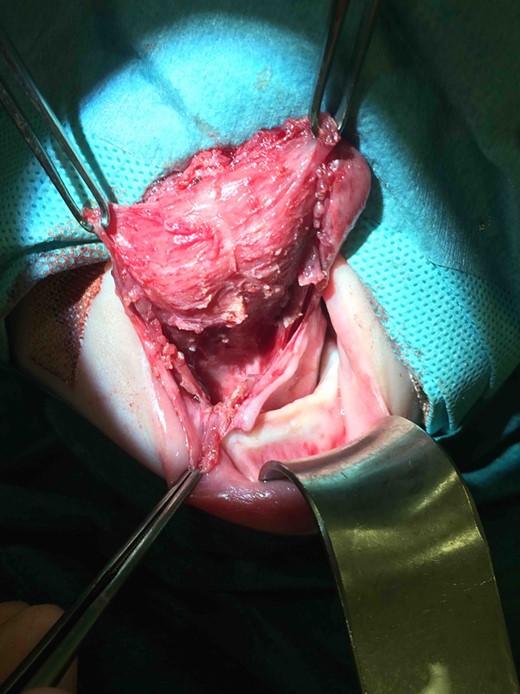
Intraoperative photograph demonstrating surgical excision of the thryoglossal duct cyst.
The postoperative course was uneventful. The baby recovered well and there has been no recurrence in the last 12 months since the operation. The baby has a normal functioning tongue, is feeding well and thriving.
DISCUSSION
TGDC are a congenital malformation which occur due to incomplete obliteration of the thyroglossal duct. In normal development, the thyroglossal duct involutes before the tenth week of gestation, however, persistence of part of the duct can lead to the development of a cyst. These can form anywhere along the path of the thyroglossal duct from the foramen caecum to the pyramidal lobe of the thyroid, however, 60% are found in the midline of the neck, between the hyoid bone and the thyroid cartilage [1, 2]. Lingual TGDCs are a rare variant, with a prevalence of 0.6–3% of all TGDCs [2]. It is thought that the rarity of the lingual subtype of TGDCs is due to the fact that involution of the thyroglossal duct commences from the cranial end [3]. Lingual TGDCs are usually located at the tongue base however interestingly in this case it was anteriorly located [4].
Lingual TGDCs are important to detect as they can cause respiratory distress or even airway obstruction in a newborn [3]. In a retrospective review of 16 patients with lingual TGDCs at a paediatric tertiary hospital, 44% presented with moderate to severe upper airway obstruction [5]. Smaller lingual TGDCs can lead to swallowing and speech difficulties [3]. In comparison to TGDCs at other locations, lingual TGDCs are more often symptomatic [4]. Early surgical intervention may be required for respiratory compromise, for diagnosis, to aid functions of the tongue such as swallowing or speech, or to prevent complications. These include acute infection, abscess formation and a small risk of malignant transformation, with 1% of TGDCs developing into carcinomas, most commonly papillary carcinoma [4].
Pre-operatively it is important to confirm the presence of a normally situated and functioning thyroid gland, as ectopic thyroid tissue could be associated with the cyst. CT or MRI scan can be useful for pre-operative planning to review the relation of the cyst to the hyoid bone, to determine the extent or in case of diagnostic uncertainty. Lingual TGDCs appear as a well-circumscribed, round, low-density lesion, most commonly at the base of the tongue [6].
As we have demonstrated with this case, aspiration of the cyst is useful for immediate symptom relief but is often associated with recurrence [7]. For definitive treatment surgical management is required. Options include transoral excision and marsupialization [8]. Sistrunk procedure is required if the cyst is situated in the neck and includes en bloch resection of the cyst, central portion of the body of the hyoid bone as well as a core of suprahyoid muscle up to the foramen caecum in the tongue base [9]. Despite this extensive resection the recurrence rate is still around 7% [10]. The extended Sistrunks procedure including a central strip of infrahyoid muscle will reduce the recurrence further [10].
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}