





Abstract
Here, we report two patients with transomental hernia who were successfully treated with laparoscopic surgery. The first patient was a 58-year-old female who presented to our hospital with abdominal pain and vomiting; she had no history of abdominal surgery. Enhanced computed tomography revealed strangulation ileus due to an internal hernia. The second patient was a 36-year-old male who presented to our hospital with abdominal pain and no history of abdominal surgery. Enhanced computed tomography indicated transomental hernia. Emergency laparoscopic surgery in both patients revealed incarcerated bowel loops through defects in the greater omentum. The bowel segments were laparoscopically released, and the patients were uneventfully discharged on postoperative Days 4 and 8. Laparoscopic surgery is useful for the diagnosis and treatment of small bowel obstruction due to transomental hernia through the greater omentum.
INTRODUCTION
Internal hernia is one of the causes of small bowel obstruction (SBO) in patients with no history of surgery. Although the incidence of internal hernia in SBO is 5.8%, transomental hernias are particularly rare, constituting only 1–4% of all internal hernias [1, 2]. Laparoscopic surgery is less invasive than laparotomy for acute bowel obstruction. We report the cases of two patients with transomental hernia through the greater omentum who were successfully treated with laparoscopic surgery.
CASE REPORT
Case 1
The first patient was a 58-year-old female who presented to our hospital with abdominal pain and vomiting; she had no history of abdominal surgery. Upon performing an examination, her abdomen was soft, with no guarding or rebound tenderness; however, central abdomen palpation revealed tenderness. A laboratory investigation revealed no abnormalities; however, enhanced abdominal computed tomography (CT) revealed intestinal obstruction of the right lower quadrant with the beak sign, indicating the transition zone of SBO (Fig. 1A). Therefore, the patient was diagnosed with strangulation ileus due to the internal hernia. Emergency laparoscopic surgery revealed an incarcerated loop of the small bowel through a greater omental defect (Fig. 2A). The incarcerated small bowel was released; because the ileal segment was viable, bowel resection was deemed unnecessary. The patient was uneventfully discharged on postoperative Day 8.
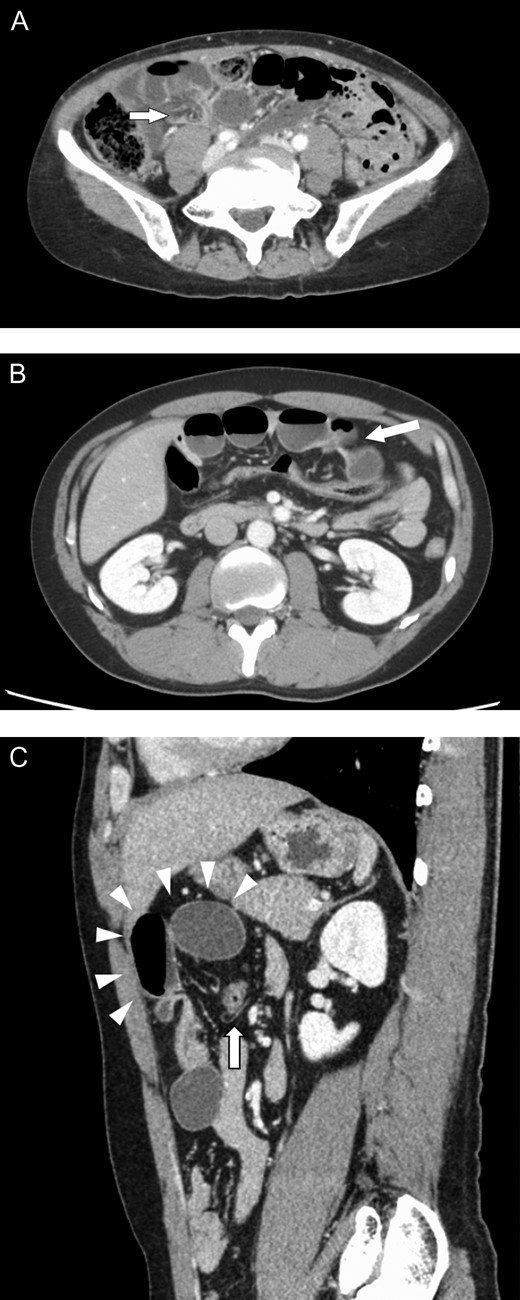
Enhanced abdominal computed tomography findings. (A) The beak sign (arrow) is indicated in the lower right quadrant. (B) Small bowel loops with caliber change (arrow) are indicated in the upper abdomen. (C) A peripheral herniated loop (arrowheads) within the peritoneal cavity. The transverse colon is indicated by an arrow.
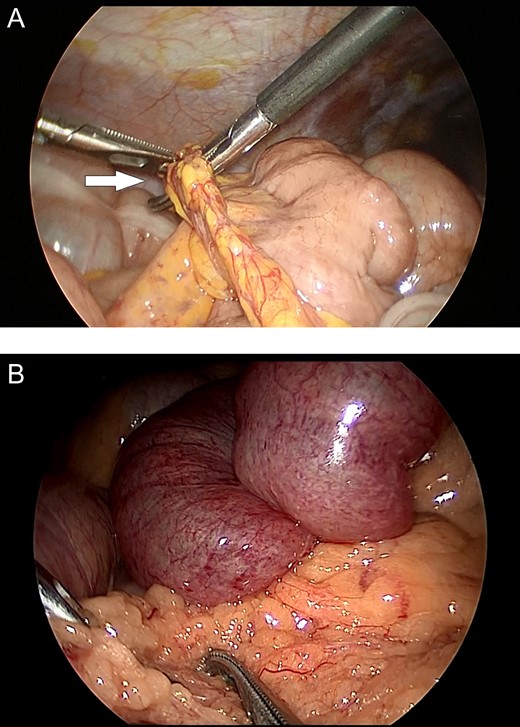
Intraoperative images. (A) Incarceration of a loop of the small bowel through a defect in the greater omentum (arrow). (B) Small bowel loops appear to be congested and herniate through the greater omentum.
Case 2
The second patient was a 36-year-old male who presented to our hospital with abdominal pain and had no history of abdominal surgery. His physical examination revealed upper abdominal tenderness. Laboratory investigations revealed no abnormalities except for an abnormal white cell count (11 000 mm3). Enhanced abdominal CT revealed dilated, fluid-filled loops of the small bowel, with caliber change in the upper abdomen (Fig. 1B and C). He was suspected of having transomental hernia, and emergency laparoscopy was performed. During surgery, an ileal segment measuring ~15 cm in length was observed to be herniating through a greater omental defect (Fig. 2B). The small bowel was released by dividing the omentum; there was no evidence of ischemic changes in the incarcerated loop of the small bowel. The postoperative course was uneventful; the patient was discharged on postoperative Day 4.
DISCUSSION
Internal hernia is a rare cause of SBO, with transomental hernia, which accounts for only 1–4% of all internal hernias, being even rarer [1, 2]. Spontaneous transomental hernia typically occurs because of senile atrophy of the greater omentum in patients with no history of abdominal surgery, trauma or inflammatory disease [3]. Symptoms can range from mild, chronic and intermittent abdominal pain to acute severe abdominal pain caused by strangulated SBO associated with nausea and vomiting. Moreover, patients with transomental hernia more frequently present with gangrenous bowel than those with other internal hernia types [4], making rapid diagnosis and treatment for avoiding bowel resection important. Although abdominal CT helps diagnose transomental hernia based on its characteristic features, the features are not universal, which makes diagnosing these hernias difficult [5]. This was exemplified in our patients, wherein the second showed classic peripheral herniated loops within the peritoneal cavity, whereas the first showed no classic features.
We searched PubMed using the keyword ‘transomental hernia’ for reports published between 1960 and 2017 and identified 24 cases, including our patients, describing herniation through the greater omentum (Table 1). The median patient age was 64.3 (range: 28–96) years; the male-to-female ratio was 12:12. Among identified patients, 16 had no history of abdominal surgery, whereas four had a history of surgery (two appendectomies, one bilateral inguinal hernia repair and one appendectomy and hysterectomy). SBO or internal hernia was preoperatively diagnosed in 12 patients; however, only two cases had diagnoses of transomental hernia based on a preoperative radiological examination. Conservative treatment of one patient resulted in death. All other patients underwent surgery and survived; only two patients experienced complications (postoperative ileus). The small bowel was herniated in 23 patients, whereas the descending/sigmoid colon was herniated in one patient. Bowel resections were required in seven patients (30.4%). The omental foramen was repaired by suture in seven patients and was divided in 13; omentectomy was performed in two patients. As indicated in Table 1, our patients were treated with laparoscopic surgery.
Review of transomental hernia cases reported in English
| No. | Authors | Year | Age | Gender | Symptom | Preoperative diagnosis | History of abdominal surgery | Operation | Bowel resection | Herniated organ | Omental foramen | Complication |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Clark PB | 1961 | 39 | Male | Abdominal pain | NA | None | Laparotomy | – | Jejunum | Divided | None |
| 2 | Clark PB | 1961 | 50 | Male | Abdominal pain, vomiting | NA | None | Laparotomy | – | Jejunum | Divided | None |
| 3 | BINNS PM | 1962 | 65 | Male | Abdominal pain | NA | NA | Laparotomy | – | Ileum | Sutured | None |
| 4 | Egan TJ | 1962 | 69 | Male | Abdominal pain, vomiting | SBO | None | Laparotomy | – | Ileum | Divided | None |
| 5 | Svane S | 1964 | 77 | Male | Abdominal pain, vomiting | None | None | Conservative | NA | Ileum | – | Dead |
| 6 | Svane S | 1964 | 63 | Male | Abdominal pain, vomiting | SBO | None | Laparotomy | – | Ileum | Sutured | None |
| 7 | Lessner KH | 1976 | 69 | Female | Abdominal pain | SBO | Appendectomy | Laparotomy | – | Ileum | Divided | None |
| 8 | Hull JD 3rd | 1976 | 67 | Female | Abdominal pain | SBO | None | Laparotomy | – | Ileum | Divided | None |
| 9 | Watt PC | 1983 | 90 | Female | Abdominal pain | NA | None | Laparotomy | + | Small bowel | Divided | Ileus |
| 10 | Siddins et al. | 1990 | 36 | Female | Abdominal pain | Sigmoid vulvulus | Appendectomy | Laparotomy | + | Descending and sigmoid colon | Sutured | None |
| 11 | Delabrousse et al. | 2001 | 87 | Female | Abdominal pain, vomitting | Internal hernia | NA | Laparotomy | + | Ileum | Sutured | None |
| 12 | Li et al. | 2005 | 91 | Female | Abdominal pain, vomiting | SBO | None | Laparotomy | – | Ileum | Divided | None |
| 13 | Yanget al. | 2009 | 74 | Male | Abdominal pain, vomiting | Internal hernia | None | Laparotomy | + | Jejunum | Sutured | NA |
| 14 | Korn et al. | 2009 | 71 | Male | abdominal pain, nausea | NA | Bilateral inguinal hernia repair | Laparotomy | – | Jejunum | Omentectomy | Ileus |
| 15 | Narjiset al. | 2010 | 30 | Female | Abdominal pain, vomiting | SBO | None | Laparotomy | – | Small bowel | Omentectomy | None |
| 16 | Choong et al. | 2010 | 46 | Male | Abdominal pain | SBO | None | Laparotomy | – | Ileum | Divided | NA |
| 17 | Le Moigne et al. | 2010 | 79 | Female | Abdominal pain | Internal hernia | None | Laparotomy | + | Ileum | Divided | None |
| 18 | Skeik et al. | 2011 | 71 | Female | Abdominal pain, vomiting | SBO | None | Laparotomy | – | Small bowel | Divided | None |
| 19 | Camera et al. | 2014 | 86 | male | Abdominal pain, vomiting | Small bowel volvulus | None | Laparotomy | + | Jejunum | NA | None |
| 20 | Tidjane et al. | 2015 | 65 | Male | Abdominal pain, vomiting | Internal hernia | None | Laparotomy | – | Small bowel | Divided | None |
| 21 | Jeffery et al. | 2015 | 28 | Female | Abdominal pain, vomiting | NA | None | Laparotomy | – | Ileum | Sutured | None |
| 22 | Malakhia et al. | 2017 | 96 | Female | Abdominal pain, vomiting | Transomental hernia | Appendectomy, Hysterectomy | Laparotomy | + | Ileum | Sutured | NA |
| 23 | Our case 1 | 2018 | 58 | Female | Abdominal pain, vomiting | Internal hernia | None | Laparoscopy | – | Ileum | Divided | None |
| 24 | Our case 2 | 2018 | 36 | Male | Abdominal pain | Transomental hernia | None | Laparoscopy | – | Jejunum | Divided | None |
Recently, laparoscopic surgery has been commonly performed for SBO [6] because of its minimal invasiveness and rapid diagnostic capability. These characteristics make laparoscopic surgery crucial for diagnosing and treating transomental hernia. In particular, the high mobility of the omentum makes detailed observation of transomental hernia possible. When risk factors such as previous abdominal surgery, trauma or peritoneal inflammation are absent in patients presenting with acute abdominal symptoms, the possibility of internal hernia should be considered, and one can expect no adhesions in the peritoneal cavity. Therefore, exploratory laparoscopy is useful for diagnosing SBO in case of SBO with high visibility. If performed early after symptom onset, laparoscopic surgery can completely save an incarcerated small bowel from necrosis. Laparoscopy offers adequate working space, given the high mobility of the omentum.
Therefore, in case of no evidence of necrosis or perforation of hernial contents, prompt laparoscopic surgery is a viable option for treating spontaneous transomental hernias.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
FUNDING
Not applicable.

{kind=link}
{kind=link}