





Abstract
Odontoid pannus or periodontoid pseudotumour is associated with a variety of rheumatological conditions. We report a case of an 80-year old man who presented with acute hydrocephalus following an emergency operation to amputate his infected left big toe. Imaging revealed a large tissue mass causing severe compression at the cervico-medullary junction and obstruction of CSF flow. The acute hydrocephalus was presumed to be related to neck manoeuvring during general anaesthesia. Following an initial emergency CSF diversion through external ventricular drainage catheter insertion, the patient subsequently underwent ventriculo-peritoneal insertion and posterior spinal decompression and fixation. To our knowledge, there have been no reported cases of tophaceous gout of the odontoid pannus causing acute hydrocephalus.
INTRODUCTION
Odontoid pannus or periodontoid pseudotumour is a well-described phenomenon. It is frequently associated with rheumatoid arthritis, however other causes of chronic atlanto-axial instability such as degenerative arthropathies and post-traumatic pseudoarthrosis of the odontoid process have been attributed to its development [1]. Complications associated with untreated odontoid pannus include cervical myelopathy, sudden death from stroke and obstructive hydrocephalus [1, 2]. We present a case of obstructive hydrocephalus precipitated by neck manoeuvring during general anaesthesia.
CASE REPORT
An 80-year-old man with a background of hypertension, gout, osteoarthritis and cerebrovascular disease presented following an injury to his left big toe. He developed confusion and sepsis secondary to deep infection of his left big toe. As part of the initial septic screen, he had a CT scan which did not show any evidence of hydrocephalus (Fig. 1a). He was started on intravenous antibiotics and the decision was made to undertake amputation of the infected toe. After extubation, he had persistently reduced level of consciousness. A CT head scan performed post-operatively showed new onset acute hydrocephalus with no evidence of haemorrhage or infarction (Fig. 1b).
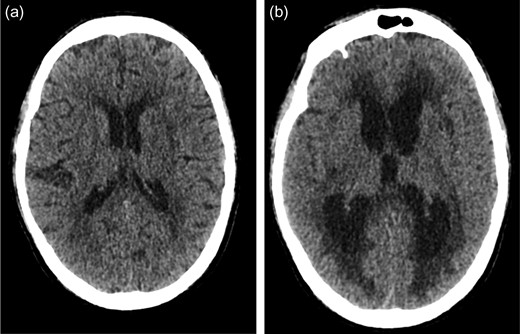
(a) Initial CT head scan performed did not show evidence of hydrocephalus. (b) Post-operative CT head showing new onset acute hydrocephalus.
He was urgently transferred to a tertiary neurosurgical centre with a GCS of 11 (E4, V2, M5) and underwent an emergency external ventricular drainage (EVD) insertion under local anaesthetic. Intra-operatively, his CSF was under moderate pressure and it was clear and colourless. His CSF results showed a white cell count of 28 × 106/L, red blood count of 3 × 106/L with no organisms. Post-operatively, he recovered to a GCS of 14 (E4, V4, M6). However, he still had persistent hydrocephalus on the repeat CT head scan. Apart from raised inflammatory markers and mild hyponatremia, his blood tests were unremarkable.
Due to crowding of his foramen magnum, a decision was made to have a MRI head and spine. This showed erosion of the odontoid with marked degenerative changes at the atlantodental joint. Interestingly, a large tissue mass presumed to be a pannus was also seen causing severe compression at the cervico-medullary junction and obstruction to CSF flow at this level (Fig. 2). Prior to this presentation, the patient had never suffered from any neck pain or limb weakness.
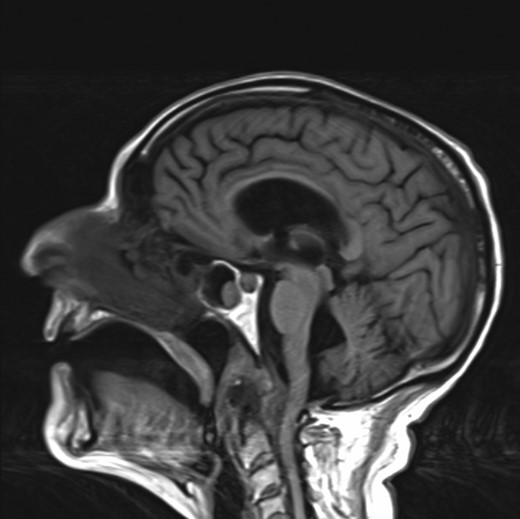
MRI head showing a large tissue mass and erosion of the odontoid causing CSF outflow obstruction at the cervico-medullary junction.
On further examination, he was not myelopathic but had widespread tophi in his hands and feet. He was started on treatment for gout with Colchicine and Allopurinol. His uric acid levels were normal at 289 umol/L. Radiographs of the hands and feet disclosed mixed osteoarthritis and gouty athropathy. He was reviewed by the Rheumatology team who felt that the odontoid pannus was most likely secondary to gout or pseudo-gout and not rheumatoid arthritis. Rheumatoid factor and anti-CCP IgG antibodies were both negative.
Due to persistent hydrocephalus on the repeat scan, he subsequently underwent ventriculo-peritoneal shunt insertion and made good recovery both cognitively and physically. The patient initially declined definitive surgical intervention and was discharged to his local hospital for ongoing rehabilitation. Following discharge to his local hospital, he developed new onset weakness in his left arm and a repeat MRI spine showed significant canal stenosis at C1 level secondary to the pannus causing cord compression.
He was transferred back to our neurosurgical unit and underwent posterior C1 and C2 decompression and C0–C3 posterior fixation. Post-operatively, he regained full power in his left upper limb and improved his mobility with physiotherapy input. He was reviewed 12 months after his initial presentation and was able to mobilize independently.
DISCUSSION
Odontoid pannus is a common pathology related to rheumatological conditions. Gout is characterized by monosodium urate deposits in articular joints and commonly affects the first metatarsophalangeal joint of the big toe, finger, elbow and knee joints [3]. Tophaceous gout affecting the axial skeleton is rare and there have only been a few reported cases of tophaceous gout affecting the atlanto-axial region. Thavarajah et al. reported a case of odontoid peg arthropathy secondary to gout which was confirmed with transoral biopsy. The patient was managed with posterior stabilization via C0–C6 occipitocervical fusion [4]. Wazir et al. [5] reported a case of tophaceous gout causing atlanto-axial subluxation mimickingrheumatoid arthrtitis that was treated via a two-stage procedure; posterior decompression and fixation followed by an anterior transoral decompression.
In our case, the odontoid pannus was thought to be probably secondary to gout or pseudo-gout as he had extensive tophi in his hands and feet. Fraser et al. [6] reported a case of confirmed tophaceous gout of the odontoid process that was managed successfully with allopurinol and colchicine alone. It is important to distinguish gouty arthropathy from rheumatoid arthritis as they may mimic one another clinically but the medical management is distinctly different [7]. Early involvement of the rheumatology team will help ensure that the appropriate medical management is initiated.
Systematic search of the Pubmed database identified no documented cases of tophaceous gout of the odontoid process causing acute hydrocephalus. However, there are cases of hydrocephalus associated with rheumatoid arthritis that have been reported in the literature [8, 9]. The pathophysiology is thought to be a structural compression of the subarachnoid space at the spinal cord level resulting in cervical myelopathy and hydrocephalus.
This case raises the question as to why he developed acute hydrocephalus during his hospital stay for management of osteomyelitis of his toe. Superior neck extension is a rare cause of hydrocephalus due to obstruction of foramen of Monro [10]. There is a possibility that the hydrocephalus was caused due to neck extension when the patient underwent intubation for surgery to amputate his left big toe as his level of consciousness reduced post-extubation. Therefore due to concerns regarding cervical spine instability, he underwent an uncomplicated fibre-optic intubation for the ventriculo-peritoneal shunt insertion procedure.
CONCLUSION
This case report demonstrates a rare cause of hydrocephalus due to pannus along the odontoid process resulting in obstructive hydrocephalus. It is an important phenomenon to be aware of in patients with odontoid pannus, particularly when performing neck manoeuvres, as it may cause obstructive hydrocephalus.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}