





Abstract
Herein we report a case of a 38-year-old men who presented with acute suprapubic pain caused by a tubular, hypoechoic, non-compressible, inguinal mass with no flow evident on color Doppler sonography. The history of the patient, the clinical signs of local inflammation and tenderness on palpation as well as the results of the Doppler ultrasound examination led to the diagnose of an inguinal hernia with bowl incarceration. However, due to a remaining uncertainty whether a bilateral or unilateral hernia was immanent and whether the bowl incarceration was caused by a right or left sided hernia the on-call surgeon initiated a computed tomography (CT) scan. Surprisingly, this CT scan revealed extensive suprapubic venous collaterals with thrombophlebitis that mimicked a bilateral inguinal hernia secondary to an acute unilateral femoral vein thrombosis. Instead of undergoing surgery the patient was treated with antibiotics, pain killer and heparin and was discharged from hospital after 8 days.
INTRODUCTION
Groin hernias have a variety of clinical presentations ranging from a bulge in the groin region on routine physical examination, to emergent presentations due to bowel strangulation. In the majority of cases diagnosis rely on the patient's history and the clinical symptoms as well as on the physical examination—without the necessity for advanced diagnostics such as computed tomography (CT) scan or magnetic resonance imaging (MRI) [1].
When the diagnosis is not apparent, imaging though can help to differentiate between inguinal hernia from other rare clinical entities [2, 3]. In most cases ultrasound is the sufficient imaging diagnostic tool, which has a high sensitivity and specificity [3] and which is noninvasive and inexpensive as well. Additional advanced diagnostics such as CT- or MRI-scans can be helpful in case of rare clinical conditions, but are usually not required and not the standard tool of differential diagnosis in inguinal pain.
The differential diagnosis of inguinal hernia includes any pathology that can produce pain or a mass within the groin region, including soft tissues infection, lymphoid tissue, associated vessels or structures associated with male or female reproduction.
CASE REPORT
A 38-year-old patient presented in the emergency room with acute suprapubic and bilateral inguinal pain. He worked as a truck driver who also was responsible for loading and unloading the truck shipments. He reported that his symptoms started with a swelling 10 days before as he had been loading and uploading shipments and was driving for long hours. He reported that his symptoms intensified significantly during the last unloading of shipments the day he presented at the emergency room. Besides bilateral inguinal pain and a tender pubic swelling with local signs of inflammation he reported no other symptoms. Nausea, fewer or intra-abdominal pain were negated. At the time of admission, the patient did not take any medicine and he had no surgical history. However, later on the patient reported about an ilio-femoral thrombosis of the right external iliacal veins and a history of an interim phenprocoumon medication.
On assessment, his temperature, heart rate and beats per minute as well as blood pressure were in the normal range. The local examination revealed a 30 cm × 15 cm sized non-reducible tender swelling in his suprapubic and bilateral inguinal regions with no cough impulse (Fig. 1). Examination of the abdomen revealed mild distension. Blood biochemistry results were as follows: hemoglobin 14.8 g/dl, white blood cell count 8300 cells/ul, creatinine 104 mmol/l, potassium 4.4 mmol/l, sodium 140 mmol/l, C-reactive protein 29 mg/l. We diagnosed an inguinal hernia with possible bowl incarceration.

As presented in the emergency room by a 38-year old patient with a tender suprapubic swelling and local signs of inflammation (rubor, calor, dolor, tumor).
For verification of the clinical diagnosis a Doppler ultrasound was performed by an experienced ultrasound examiner. In the ultrasound a hernia with prolapsed intestine was diagnosed due to a tubular, hypoechoic, non-compressible, inguinal mass with no flow evident on color Doppler imaging (Fig. 2). However, it was unclear whether the hernia was caused by a bilateral or unilateral gap. Only for surgery planning purposes we decided to perform a CT scan to identify the side of the gap and classify the kind of hernia (direct/indirect). Surprisingly the CT scan showed large venous collaterals between left and right Vena femoralis and a illio-femoral thrombosis on the left side. No inguinal or any other hernia of the suprapubic and inguinal regions were found (Fig. 3). The venous collaterals showed extensive signs of inflammation—concordant with the diagnosis of a local suprapubic thrombophlebitis. After the CT scan the patient was re-evaluated by Doppler ultrasound. Knowing the CT scan results and by readjustment of Doppler settings that diagnosis was confirmed.
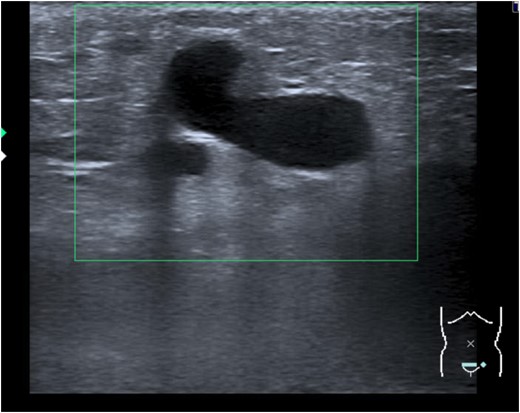
Tubular, hypoechoic, non-compressible, inguinal mass with no flow evident in color Doppler imaging.
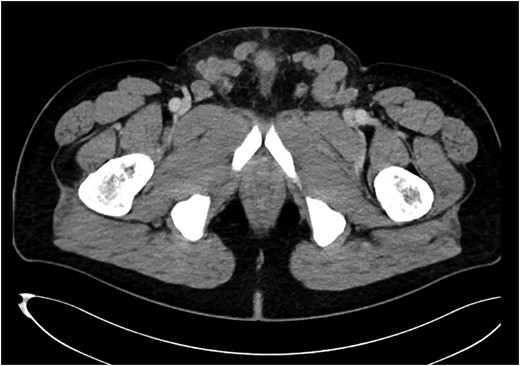
A CT-abdomen revealed suprapubic crossover collaterals due to ilio-femoral vein occlusion secondary to DVT.
The patient was then admitted to the internal medicine ward and treated with ibuprofen, antibiotics, low-molecular-weight heparin and cool packs. He continued to improve and was discharged 8 days later. A reason for the thrombosis such as a malignancy, coagulation defect or any other hematologic diseases could not be detected. The thrombosis was most likely caused by a continued hip flection with venous compression and venous kinking leading to venous blood flow stagnation and consecutive thrombosis during non-stop steering hours as a long-distance truck driver.
DISCUSSION
Suprapubic crossover collaterals as clinical signs for a left iliac vein obstruction are an uncommon presentation in adults. The sonographic appearance mimicked a hernia by demonstrating a tubular, hypoechoic, non-compressible, inguinal mass with initially no flow evident on color Doppler imaging due to partial thrombosis of the venous collaterals. Further due to the thrombophlebitis of these aberrant vessels the patient presented with acute suprapubic pain and therefore the diagnosis of an acute inguinal hernia seemed to be obvious. However, the side of the hernia remained unsure und in order to better plan the operation a CT scan was performed with the reported unexpected result.
In the literature thrombosis of the pampiniform plexus has been misdiagnosed as an incarcerated inguinal hernia [4] and we could also find a single further case of suprapubic crossover collaterals in the combination with thrombophlebitis simulating a inguinal hernia reported by Davey et al. [5].
Pubic collateral veins can be a clinical sign of iliac vein occlusion, e.g. secondary to deep vein thrombosis (DVT). They can develop via enlarged external pudendal, superficial epigastric and superficial circumflex iliac veins. Finally concerning the therapy of acute thrombophlebitis non-steroidal anti-inflammatory agents (NSAIDs) are effective in relieving the pain associated with venous inflammation and the American College of Chest Physicians suggests anticoagulation for patients at increased risk for thromboembolism. However, the best agent, dose and duration of anticoagulant medication remain unclear [6].
Suprapubic crossover collaterals are an unusual cause for an acute inguinal pain. Although Doppler ultrasound has a high sensitivity and specificity for distinguishing hernia from other inguinal and scrotal pathologies, in some cases (e.g. thrombosis of the collaterals with consecutive thrombophlebitis), such collaterals can mimic inguinal hernia and mislead to wrong therapeutic strategies.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}