Abstract
Cancer of unknown primary (CUP) is a well-known entity that can present in a multitude of clinical presentations. Based on the extent and organ of involvement, the presentation will be varied. For instance, patients presenting with axillary lymphadenopathy would lead toward a primary breast cancer, whereas patients presenting with abdominal distention due to ascites would tend toward a gastrointestinal origin. We present a case of a 73-year-old female who presented with an abdominal wall mass; on laparoscopy, she was found to have a spigelian hernia due to an omental metastatic lesion from a CUP.
INTRODUCTION
Cancer of unknown primary (CUP) is a well-recognized clinical disorder, accounting for 3–5% of all malignant epithelial tumors [1]. It is characterized as an aggressive disease with an early dissemination of metastases without a primary detected site after extensive laboratory and clinical investigations [2]. The National Comprehensive Cancer Network (NCCN) have set forth guideline for work-up based on clinical presentation, with all including extensive history and physical exam, computed tomography (CT) of chest/abdomen/pelvis and site/gender-specific diagnostic studies (i.e. mammogram and testicular US) and tumor markers (i.e. CA-125 and prostate specific antigen [PSA]), as well as appropriate immunohistochemistry.
CASE REPORT
A 72-year-old female with a history of chronic headaches and osteoarthritis, as well as surgical history of total abdominal hysterectomy and bilateral salpingo-oopherectomy (SOO) due to ovarian cysts and dysmenorrhea, presents to her primary care with complaints of pain in the left side of her abdomen and feeling a lump in that location for the past 7–10 days. She stated that she had never noticed the lump and the pain started abruptly. She denies any fever, night sweats or weight loss. On physical exam, she was found to have a bulge on the left side of the abdomen just lateral to the rectus muscle, it was firm and immobile and appeared to be outside the abdominal wall. She was sent for a CT scan of the abdomen and pelvis, which showed a hernia and was suggestive of carcinomatosis with omental and parietal implants. She was referred to a general surgeon and was scheduled for a diagnostic laparoscopy and an esophagogastroduodenoscopy (EGD). Her EGD was completely normal, but on her diagnostic laparoscopy she was noted to have diffuse tumor implants along the liver, diaphragm, peritoneum and omentum (Figs
1 and
2). The largest omental implant measuring ~3 × 4 cm was herniated through the semilunar line of the abdominal fascia causing a spigelian hernia (Fig.
3). Biopsies of the peritoneal and omental implants were obtained. It was decided to leave the hernia due to the size of the defect and requirement for a large mesh for repair in a cancer riddled abdomen that may be re-entered for debulking. The pathology report returned as metastatic adenocarcinoma of unknown origin. The cancer stained diffusely positive for CK7 and CK20; suggestive of gastrointestinal, pancreatic, biliary or ovarian origin, less likely pulmonary origin. Her pathology report from her prior SOO was pulled and compared and showed both ovaries were benign serous cystadenoma and histologically no similarity between the patient’s resected ovarian tumors and the current omental implants was noted. She underwent CT chest/brain, colonoscopy, mammogram and CA 19-9 level; all returned normal. She underwent a Positron emission tomography (PET) scan as well and only the known abdominal masses were suggestive of cancer. Decision was made to treat the patient as primary peritoneal malignancy with a platinum-taxane based chemotherapy regimen. A subcutaneous port was placed and the patient was discharged and started on chemotherapy.
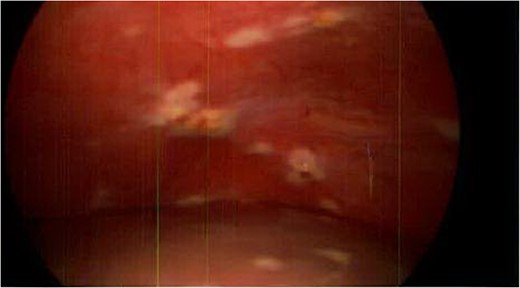
Figure 1:
Liver and peritoneum with metastatic implants.

Figure 2:
Omental metastatic lesion.

Figure 3:
Spigelian hernia. Omental metastatic lesion protruding through the semilunar line.
DISCUSSION
CUP is divided into two subsets, favorable (20%) and unfavorable (80%), based on histopathology and clinical presentation (Table 1). About 80% of cases that are first diagnosed as CUP eventually have a confirmed type. Roughly 60% of CUP primary sites are adenocarcinomas arising from glandular cells (lung, pancreas, breast, prostate, stomach, colon and liver) while the remaining sites of origin include melanoma, sarcoma, lymphoma and neuroendocrine tumors [3]. Patient presentation varies depending on the location of metastasis. Common presentations are non-specific such as non-tender swollen lymph nodes, palpable mass in the abdomen, pain in the bones and unexplained weight loss. Patients with carcinoma of unknown primary site are heterogeneous with respect to tumor biology, clinical characteristics and response to therapy. Extensive work-up with specific pathology investigations (immunohistochemistry, electron microscopy, molecular diagnosis) and modern imaging technology (CT, mammography and PET scan) have resulted in some improvements in diagnosis; however, the primary site remains unknown in most patients, even on autopsy [4]. Subsequent evaluation and treatment differ depending on the classification of CUP. In our case, the patient has a mixed favorable and unfavorable profile since she has a cancer that closely resembles a colonic origin, but presented with liver metastasis.
| Favorable subsets
. | Unfavorable subsets
. |
|---|
| 1.Women with adenocarcinoma involving axillary lymph nodes | 1. Adenocarcinoma metastatic to the liver or other organs |
| 2. Women with papillary carcinoma involving the peritoneal cavity | 2. Poorly differentiated carcinoma |
| 3. Squamous cell carcinoma involving cervical lymph nodes | 3. Non-papillary malignant ascites (adenocarcinoma) |
| 4. Poorly differentiated neuroendocrine carcinomas. Merkel cell carcinoma of unknown primary (localized disease) | 4. Multiple cerebral metastasis (adeno or squamous carcinoma) |
| 5. Adenocarcinoma with a colon profile (CK20+, CK7−, CDX2+) | 5. Multiple lung/pleural metastasis (adenocarcinoma) |
| 6. Isolated inguinal adenopathy (squamous carcinoma) | 6. Multiple metastatic bone disease (adenocarcinoma) |
| 7. Men with blastic bone metastasis and elevated PSA (adenocarcinoma) | 7. Squamous cell carcinoma of the abdominal cavity |
| 8. Patients with a single, small, potentially resectable tumor |
| Favorable subsets | Unfavorable subsets |
|---|
| 1.Women with adenocarcinoma involving axillary lymph nodes | 1. Adenocarcinoma metastatic to the liver or other organs |
| 2. Women with papillary carcinoma involving the peritoneal cavity | 2. Poorly differentiated carcinoma |
| 3. Squamous cell carcinoma involving cervical lymph nodes | 3. Non-papillary malignant ascites (adenocarcinoma) |
| 4. Poorly differentiated neuroendocrine carcinomas. Merkel cell carcinoma of unknown primary (localized disease) | 4. Multiple cerebral metastasis (adeno or squamous carcinoma) |
| 5. Adenocarcinoma with a colon profile (CK20+, CK7−, CDX2+) | 5. Multiple lung/pleural metastasis (adenocarcinoma) |
| 6. Isolated inguinal adenopathy (squamous carcinoma) | 6. Multiple metastatic bone disease (adenocarcinoma) |
| 7. Men with blastic bone metastasis and elevated PSA (adenocarcinoma) | 7. Squamous cell carcinoma of the abdominal cavity |
| 8. Patients with a single, small, potentially resectable tumor |
CUP is a clinical entity that is not as uncommon as previously thought. As our patients’ CUP presented as a spigelian hernia this is quite a rare occurrence. Spigelian hernias are anterior abdominal wall hernias that occur at a defect adjacent to the semilunar line and they comprise only 0.12% of all abdominal wall hernias and are difficult to diagnose clinically depending on its location [5]. Though rare concomitant disease processes, CUP as a spigelian hernia should be included in the differential diagnosis of anterior abdominal wall masses, even in the absence of symptoms suggestive of cancer.
CONFLICT OF INTEREST STATEMENT
None declared.
REFERENCES
1Pavlidis
N
, Pentheroudakis
G
.
Cancer of unknown primary site
.
Lancet
2012
;
379
:
1428
–
35
.
2Pavlidis
N
, Khaled
H
, Gaafar
R
.
A mini review on cancer of unknown primary site: a clinical puzzle for the oncologists
.
J Adv Res
2015
;
6
:
375
–
82
.
3Pavlidis
N
, Briasoulis
E
, Hansworth
J
, Greco
F
.
Diagnostic and therapeutic management of cancer of an unknown primary
.
Eur J Cancer
2003
;
39
:
1990
–
2005
.
4Benderra
M
, Ilie
M
, Hofman
P
, Massard
C
.
Standard of care of carcinomas on cancer of unknown primary site in 2016
.
Bull Cancer
2016
;pii: S0007-4551 (16) 30084-4.
5Mittal
T
, Kumar
V
, Khullar
R
, Sharma
A
, Soni
V
, Baijal
M
, Chowbey
P
.
Diagnosis and management of Spigelian hernia: a review of literature and our experience
.
J Minim Access Surg
2008
;
4
:
95
–
8
.
Published by Oxford University Press and JSCR Publishing Ltd. All rights reserved. © The Author 2017.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/), which permits non-commercial re-use, distribution, and reproduction in any medium, provided the original work is properly cited. For commercial re-use, please contact journals.permissions@oup.com







{kind=link}