Abstract
The adolescent avulsion of the lesser tuberosity of the humerus has historically been considered as very rare. The youngest patient reported in the literature is 11 years old. We report a case of a 9-year-old girl who suffered a subscapularis tendon tear with an occult avulsion of the lesser tuberosity. Late repair restored function. Despite that late repair in this present case resulted in excellent outcome, we strongly recommend the additional axillary lateral view of the plain radiographs, as well as proper physical examination to facilitate early diagnosis.
INTRODUCTION
Various avulsion fractures occur in pediatric patients. Avulsion of the anterior tibial tuberosity, the medial epicondyle of the humerus and the anterior superior iliac spine are some of the most common [1]. Rotator cuff tears are rare in the pediatric population. In skeletally immature patients, subscapularis injuries are to our knowledge always associated with an avulsion of the lesser tuberosity in varying size. The lesion is often a type of a periosteal sleeve fracture and if the avulsion fragment is small or consist of periosteum only, the diagnosis might go undetected. The plain radiographs together with the radiological report could mislead the emergency care doctor to interpret the injury as a simple strain.
CASE REPORT
A 9-year-old female swimmer suffered a forceful external rotation–abduction injury of her right shoulder while falling on a slippery swimming arena floor. The primary care doctor ordered plain radiographs due to limited active range of motion and anterior shoulder tenderness. The radiological report was negative. The patient could not return to swimming and other sport activities and were treated by a physical therapist for several months. Because of persistent weakness and increasing internal rotation deficit, she was referred to our department 1-year after the injury. Clinical examination was inconclusive and plain radiographs and magnetic resonance imaging (MRI) arthrogram was ordered (Fig.
1).
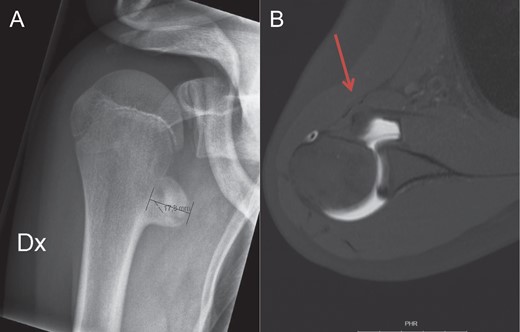
Figure 1:
Anteroposterior view of the right shoulder (A) shows the exostosis localized inferior and medial to the origin of the native lesser tuberosity. On the transverse view of the arthro MRI (B), the anteriorly displaced subscapularis tendon due to the new insertion site on the exostosis, is marked with the red arrow.
The radiographs showed a metaphyseal exostosis and the arthro MRI revealed no signs of other than benign bone mass. The radiographs from the injury event were re-reviewed. Now, with this new information, the diagnosis was clear. The small fragment of the periosteal sleeve fracture was detectable (Fig.
2).

Figure 2:
Axillary lateral view of the injured right shoulder. The avulsion fragment of the lesser tuberosity is marked by the red arrow.
Despite the meticulous rehabilitation, the girl complained of persistent weakness of her shoulder in addition to lack of internal rotation. The physical examination revealed full forward flexion, abduction and extern rotation but ~30° deficits in internal rotation. The exostosis was palpable and there was a popping sensation over the exostosis during rotation of the humerus. Belly-press and lift-off tests were both positive. Fifteen months after the traumatic event she underwent excision of the exostosis with reattachment of the subscapularis tendon to its original footprint.
In a beach chair position, a standard deltopectoral approach was undertaken (Fig.
3A) and the thumblike bony mass with the attached subscapularis tendon was dissected free (Fig.
3B). The long head of the biceps was macroscopically intact in the bicipital groove. A small fragment assimilating the size of the native lesser tubercle, together with the intact subscapularis tendon and the anterior capsule, was osteotomized off the bony mass. The rest of the bony mass was excised. Interestingly, the upper one-eighth of the subscapularis tendon was intact and identified the superior border of the native footprint. The rest of the footprint was decorticised and a Fast in RC anchor (DePuy Mitek, Warsaw, Indiana) with two mattress sutures was utilized to secure the capsule and tendon just lateral to the cartilage margin and act as a medial row for the tubercle fixation (Fig.
3C). Drill holes medial and lateral to the bicipital groove completed the transosseous fixation with the sutures bridging the lesser tubercle and going underneath the intertubercular groove leaving the tendon and tendon sheath uninjured (Fig.
3D).
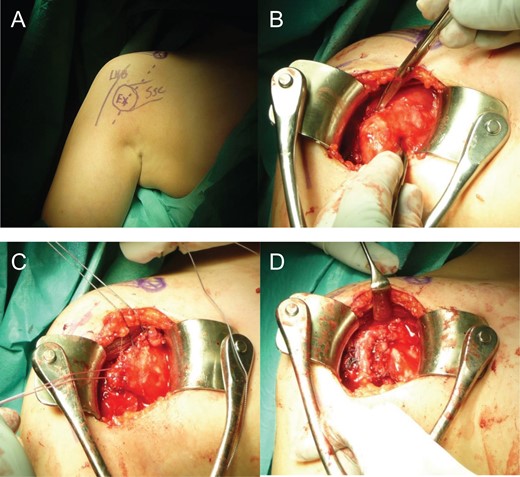
Figure 3:
Open repair of the subscapularis tendon with a suture bridging technic leaving the uninjured long head of the biceps intact. The standard deltopectoral incision goes directly over the palpable bony mass developed after endostal hematoma ossification (A). Almost the complete subscapularis tendon was attached to the bony mass (B). After osteotomizing the tendon insertion, the tendon including the underlying anterior capsule, was dissected free (C) and secured back to anatomic position using suture bridging technic (D).
The patient was put in a sling for 4 weeks and was allowed passive range of motion with forward flexion to 135°, abduction with neutral rotation to 90° and external rotation to 45°. After 4 weeks the sling was removed and full active assisted training was started. Resisted training of the subscapularis tendon was allowed after 8 weeks. The rehabilitation under supervision of a physical therapist was successful and the girl restored her shoulder function at 5 months post-operatively and returned to the same swimming competing level as pre-injury. One year after surgery the final follow-up was undertaken, including MRI. The subscapularis tendon appeared normal concerning both size and position, so as the quality and quantity of the muscle belly (Fig.
4). The physical examination revealed full forward flexion, abduction and extension and a 5° deficit of internal and external rotation was noted. The patient continued to be asymptomatic.
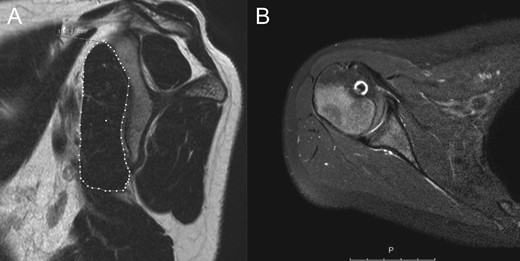
Figure 4:
MRI 1-year after surgery. In the sagittal view there are no sign of atrophy or fatty infiltration of the subscapularis muscle (A). The subscapularis tendon is healed in an anatomical position (B).
DISCUSSION
Traumatic rotator cuff tears occur mostly in middle-aged men with inferior tendon quality due to degeneration and tendon weakness [2]. Strong, healthy tendons, as in adolescents, typically resist even excessive force and the weaker link of the chain, the apophysis including the periosteum avulse from the bone [3]. Most authors advocate surgical treatment because of the high risk of impaired shoulder function after missed or delayed diagnosis [4, 5].
The few reports in the literature support the theory postulated by Vezeridis et al. [6], that these injuries are ‘transitional’ fracture in the skeletally immature adolescents. According to Goeminne et al. [7], the injury is most frequent between the age of 12 and 14 and there are only two published cases of avulsion fracture of the lesser tuberosity among female adolescents. To the best of our knowledge, the youngest patient reported was 11 years old at the time of the injury.
Even though late repair, as in this present case and other published cases [5, 8–10], could restore function and provide excellent outcome, more attention should be given to early diagnosis. This would prevent prolonged impairment of the shoulder function and the inability to continue with sport activities. Proper physical examination combined with plain radiographs including the axillary lateral view should lead to a strong suspicion of this lesion which is best confirmed by MRI or computed tomography arthrogram.
In conclusion, occult avulsion fracture of the lesser tubercle is very rare and early diagnosis is challenging. Axillary lateral view radiographs together with proper physical examination should lead to suspicion. However, by late diagnosis, delayed repair may restore function.
ACKNOWLEDGEMENT
The study was supported by grants from Stig og Ragna Gorthon Research Foundation, Helsingborg, Sweden.
CONFLICT OF INTEREST STATEMENT
The author has no conflict of interest to report and have received no financial or material support related to this manuscript.
CONSENT
The patient and her parents have given their informed consent for publishing this case report.
REFERENCES
1Stevens
MA
, El-Khoury
GY
, Kathol
MH
, Brandser
EA
, Chow
S
.
Imaging features of avulsion injuries
.
Radiographics
1999
;
19
:
655
–
72
.
2Mall
NA
, Lee
AS
, Chahal
J
, Sherman
SL
, Romeo
AA
, Verma
NN
, et al. .
An evidenced-based examination of the epidemiology and outcomes of traumatic rotator cuff tears
.
Arthroscopy
2013
;
29
:
366
–
76
.
3Ramachandran
M
, Skaggs
D
. Physeal injury. In: Green
NE
, Swiontkowski
MF
.
Skeletal Trauma in Children
. 4th ed.
Philadelphia, PA
:
Saunders
,
2009
;
19
–
40
.
4Klasson
SC
, Vander Schilden
JL
, Park
JP
.
Late effect of isolated avulsion fractures of the lesser tubercle of the humerus in children. Report of two cases
.
J Bone Joint Surg Am
1993
;
75
:
1691
–
4
.
5Kunkel
SS
, Monesmith
EA
.
Isolated avulsion fracture of the lesser tuberosity of the humerus: a case report
.
J Shoulder Elbow Surg
1993
;
2
:
43
–
6
.
6Vezeridis
PS
, Bae
DS
, Kocher
MS
, Kramer
DE
, Yen
YM
, Waters
PM
.
Surgical treatment for avulsion injuries of the humeral lesser tuberosity apophysis in adolescents
.
J Bone Joint Surg Am
2011
;
93
:
1882
–
8
.
7Goeminne
S
, Debeer
P
.
Case report: the natural evolution of neglected lesser tuberosity fractures in skeletally immature patients
.
J Shoulder Elbow Surg
2012
;
21
:
6
–
11
.
8Echlin
PS
, Plomaritis
ST
, Peck
DM
, Skopelja
EN
.
Subscapularis avulsion fractures in 2 pediatric ice hockey players
.
Am J Orthop (Belle Mead, NJ)
2006
;
35
:
281
–
4
.
9Ogawa
K
, Takahashi
M
.
Long-term outcome of isolated lesser tuberosity fractures of the humerus
.
J Trauma
1997
;
42
:
955
–
9
.
10Paschal
SO
, Hutton
KS
, Weatherall
PT
.
Isolated avulsion fracture of the lesser tuberosity of the humerus in adolescents. A report of two cases
.
J Bone Joint Surg Am
1995
;
77
:
1427
–
30
.
Published by Oxford University Press and JSCR Publishing Ltd. All rights reserved. © The Author 2017.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/), which permits non-commercial re-use, distribution, and reproduction in any medium, provided the original work is properly cited. For commercial re-use, please contact journals.permissions@oup.com







{kind=link}
{kind=link}
{kind=link}
{kind=link}