





Abstract
Differentiated carcinomas of the thyroid gland usually have a good prognosis with prognosis often discussed in terms of 20 year survival. Nevertheless its 10-year-survival rate decreases when accompanied by distant metastasis. Follicular thyroid cancer (FTC) is the second most common thyroid cancer and usually presents with a solitary thyroid nodule with or without cervical lymphadenopathy. Distance metastasis at initial diagnosis is seldom observed with incidence range from 1 to 9%. In cases of bone metastasis, the incidence is only 2–3% and weight-bearing skeleton is preferentially affected. In our case, we present a patient with FTC that metastasized to the upper limb causing severe pain and pathological fracture at the initial presentation.
INTRODUCTION
Follicular carcinoma of thyroid gland is the second most common thyroid cancer after papillary thyroid carcinoma. Clinically, differentiated thyroid cancer (DTC) commonly presents with a solitary thyroid nodule and/or cervical lymphadenopathy. Distant metastasis at initial presentation, especially those involving bone, is seldom seen and associated with poor clinical outcomes. In those cases, the axial skeleton and in particular the spine and the ribs are preferentially involved resulting symptoms such as severe pain and compression fracture [1, 2]. A pathological fracture of the upper limb as an initial symptom of a late diagnosis of DTC is therefore extremely rare and has almost never been reported in literature. In this paper, we present a case of a patient with follicular thyroid cancer who presented with pathological fracture of the humerus without preceding illness.
CASE REPORT
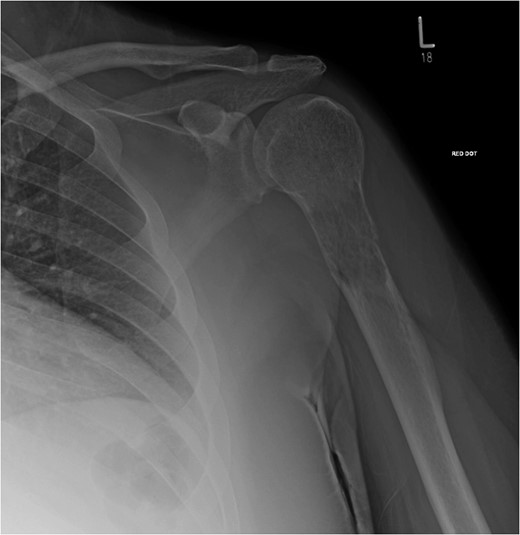
X-ray showed lytic lesion and pathological fracture of left proximal humerus. Plain radiographs of the left.
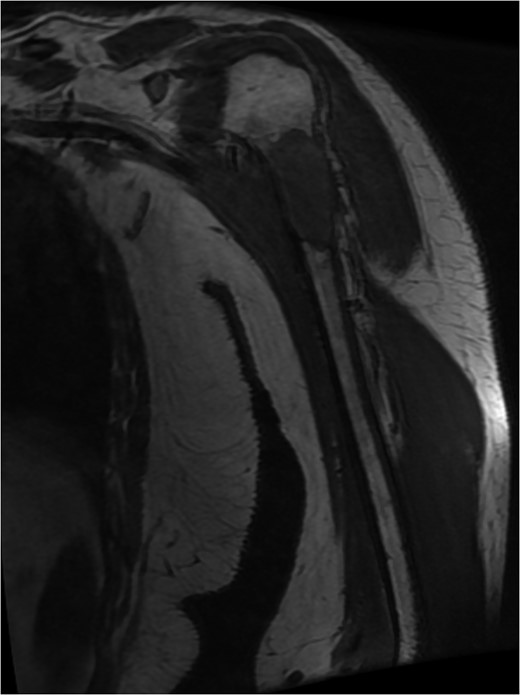
MRI left humerus showed pathological fracture of the neck and proximal shaft humerus, measure 6 × 2.5 × 2.8 cm in maximal dimension. An urgent staging magnetic resonance.
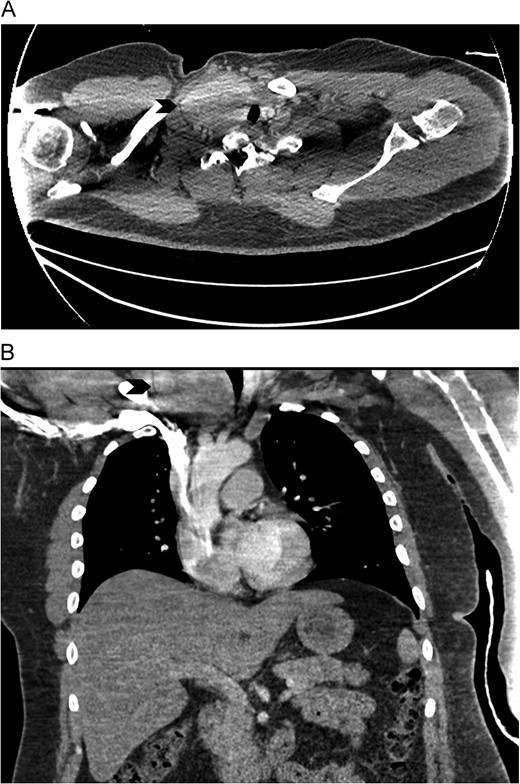
CT Chest with contrast showed an enlarged right lobe thyroid gland with retrosternal extension causing compression and deviation of trachea (arrow). (A) axial view. (B) coronal view. CT scan.
The thyroid lobe was investigated 6 years before where a multi-nodular goitre (MNG) with a dominant solitary nodule on the right thyroid lobe was discovered. Ultrasound did not show any suspicious characteristics. A fine needle aspiration cytology (FNAC) specimen of the solitary nodule was reported as a Thy2 with features consistent with a simple nodule. The investigations were arranged by the patient's general medical practitioner who reassured the patient without the input of secondary services.
Following the finding of the CT scan, the patient was referred to the local ENT department, where ultrasound of the neck and core biopsy of the thyroid nodule was conducted. The image confirmed a MNG with largest nodule in the right lobe. And the core biopsy showed a follicular pattern with thyroid follicles of varying sizes set in a mixture of fibrous tissue.
A CT guided biopsy of the left humerus after the initial presentation confirmed a metastatic thyroid cancer.
The patient underwent urgent excision of tumour and replacement of left proximal humerus. Histologically, the mass from the left proximal humerus demonstrated features consistent with metastatic thyroid carcinoma. Six weeks later, he underwent total thyroidectomy and neck dissection. A large thyroid lobe was found with no local invasion and four large Level VI lymph nodes were excised. The pathologic findings confirmed complete excision of a 70 mm widely invasive follicular carcinoma with evidence of vascular invasion and metastasis of three out of the four central neck nodes.
After thyroidectomy, the patient was seen by clinical oncology and radioiodine therapy was administered. He continues to be followed up by the local orthopaedic and ENT teams.
DISCUSSION
Patients with bone metastases of unknown origin are not uncommon in clinical practice. The primary tumour is most likely found in breast and prostate followed by the thyroid gland [3]. The bone metastases in DTC is osteolytic in nature and its distribution preferentially involves the weight-bearing skeletons such as vertebrae (52.5%), femur (20.4%), pelvis (16.0%) and clavicle (13.6%) [4]. Common manifestations of the osseous metastases include pain, fracture and spinal cord compression associated with lesion in the axial skeleton. In this case, we described an extremely rare scenario where pathological fracture of the upper limb was the initial presentation of metastatic DTC.
Of interest in our case is that the patient presented with a thyroid lump 6 years before which was diagnosed as a dominant nodule with a background of benign MNG. In the absence of suspicious sonographic ultrasound features and benign pathocytological finding of Thy2 on FNAC, the patient was reassured by the general practitioner. Although ultrasound-guided FNAC is an excellent tool for evaluating patients with solitary thyroid nodules, its utility in patients with MNG has been questioned in the past [5]. The British Thyroid Association (BTA) recommends FNAC should be carried out if ultrasound features are equivocal, indeterminate or suspicious of malignancy [6]. In our case, FNAC was performed although the nodule appeared benign and subsequent FNAC result supported the findings that the nodule was benign in nature. Despite this, our patient presented with a malignancy 6 years later. In cases where FNAC were conducted and proven to be benign in patients with non-functional, cervical MNG the incidental thyroid cancer discovered at the time of thyroidectomy can be as high as 23% [5]. Male gender tends to be associated with an increased likelihood of cancer on final pathology [5, 7].
In conclusion, despite the relative rarity of causing pathological fracture in the humerus, thyroid cancer should be considered during assessment of the patient with pathological fractures of unknown primary origin. Although the gold standard for investigation thyroid nodule remains ultrasound-guided FNAC, a benign FNAC especially in male patients with a MNG may need a more aggressive management due to the increased risk of an undetected thyroid cancer.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}