





Abstract
Anomalous origin of the coronary arteries is a rare congenital heart defect that may lead to disturbed life style, myocardial infarction and sudden death. This report describes a young lady with the right coronary artery arising from the left main coronary artery, which was confirmed by coronary angiography and corrected surgically using saphenous vein patch.
INTRODUCTION
Congenital anomalies of the coronary arteries appear in coronary angiography with an approximate incidence of 0.6–1.3%. Of these, 90% are abnormalities of the origin of the coronary arteries, and the rest are coronary artery fistulas [1, 2]. We report a case of right coronary artery (RCA) arising as a proximal branch of the left main coronary artery (LMCA) near the left sinus of Valsava, which was confirmed by coronary angiography and surgically repaired by RCA reimplantation into the right sinus of Valsava using saphenous vein patch (SVP).
CASE REPORT
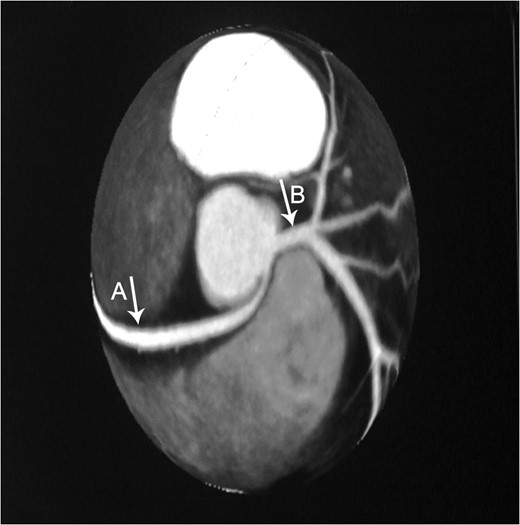
Axial CTA demonstrates an anomalous origin of RCA (Arrow A) which arises as a branch from LMCA (Arrow B).
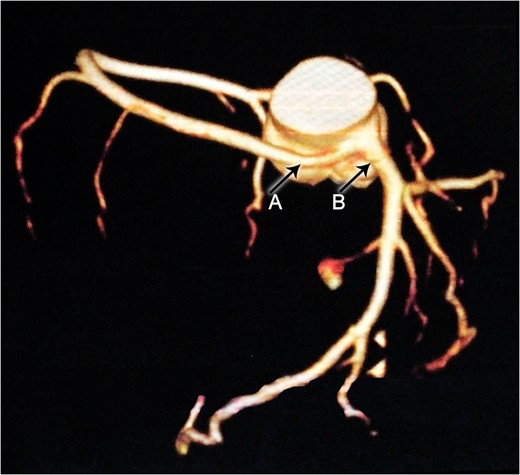
Constructional CT demonstrates an anomalous origin of RCA (Arrow A) which arises as a branch from LMCA (Arrow B).
The patient was counseled with the surgical correction, and the consent form was signed by her. A median sternotomy was performed, and mild hypothermic (35°C) cardiopulmonary bypass was started. After exposing the left artery and RCA, we found that the origin of the RCA originated from the left sinus of Valsalva. The RCA was dissected from its attachment to the left main at the left sinus of Valsalva. Partial aortic cross-clamp was applied. Small longitudinally aortotomy was done. The SVP measuring 1.5 × 2 cm2 sewn to the ascending aorta, the RCA reimplanted into the SVP using 7-0 polypropylene continuous suture forming neo-ostium of the RCA. SVP used to decrease the risk of retraction at the anastomotic site. The perioperative course went smoothly. Over the past 3 years’ serial follow-up visits in the outpatient clinic, the patient is asymptomatic and performing her life activities perfectly well.
DISCUSSION
Congenital coronary artery anomalies are present in ~0.6–1.3% of adults undergoing coronary angiography and rarely involve the RCA [2]. Anomalous origin of RCA from the LMCA is an infrequently encountered condition [3].
Most patients with RCA anomalous origin are young and otherwise healthy. However, it is associated with variable clinical presentations, the extremes of which are no symptoms to sudden death, having in between easy fatigability, angina pectoris and myocardial infarction in the absence of atherosclerosis [4].
This previously asymptomatic 37-year-old patient presented with continuous complaints of dyspnea on exertion associated with chest pain. Making her candidate for CTA which demonstrated the very rare anomalous origin of the RCA as a proximal branch from the LMCA that then continues between the pulmonary artery and ascending aorta where it is slightly compressed during systole. This finding provides us with the explanation of the presenting symptoms of such a case, which is supported by Grollman et al. ateriographic study [5].
Conservative treatment was proposed in Japan as a main line of treating patients with anomalous origin of coronary arteries. This includes limitation of exercise and drug therapy (such as nitrates, calcium channel blockers, B-adrenergic antagonists and antiarrhythmics) showing an apparent improvement in 69.2% [6].
Surgical treatment should aim at restoring the normal anatomical position of RCA to the original right ostium. However, the used surgical technique of choice is still controversial. Literature review suggests several different approaches, including coronary artery bypass, coronary reimplantation and unroofing of the intramural segment (also termed as osteoplasty) [4, 7, 8].
In the 1980s, Bett et al. used a single saphenous vein graft inserted from the aorta to the RCA as it emerged from behind the pulmonary artery [9]. Reul et al. reported patients who underwent ligation of the anomalous coronary artery and bypass with a saphenous vein graft, and others where the right internal mammary artery graft had been used without ligation of the RCA [10].
The present case was treated by RCA reimplantaion using the SVP, measuring 1.5 × 2 cm2, aiming at preventing future stenosis at the site of reimplementation. According to the literature, this exact use of saphenous patch was not used before in the surgical therapy of RCA anomalous origin. However, this has been introduced in surgical treatment of other coronary artery diseases; Kuwaki et al. who used an SVP for the reconstruction of left anterior descending coronary artery aneurysm [11], and Raffa et al. reported a case in which an SVP plasty was used in the surgical therapy of LMCA ostial disease [12].
In conclusion, anomalous origin of the RCA as a proximal branch from LMCA is very uncommon. Long-term studies on the surgical repair techniques are needed, which will help in early identifying of such cases and decreasing the mortality of lately managed cases.
ACKNOWLEDGEMENT
We would like to thank Laura Knott, M.D. Baylor College of Medicine, for her efforts in reviewing our paper.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.

{kind=link}