





Abstract
Colorectal Carcinoma is the second biggest killer after lung and bronchial carcinoma. Due to its insidious onset and late manifestation of symptoms a national screening programme was started in 2006 within the UK. We present a rare case of colorectal adenocarcinoma mimicking osteosarcoma and presenting as hip pain at initial consultation in the orthopaedic clinic. Further adding to the rarity of this case is that of an apparent bony metastasis in isolation. Our case demonstrates the vital role that histological sampling plays in the diagnosis and treatment of carcinomatous disease. It also demonstrates the need to maintain high index of clinical suspicion, no matter how benign the presenting complaint may seem.
Introduction
Colorectal carcinoma (CRC) is the third most common type of cancer in adults and is responsible for the second highest incidence of death after lung and bronchial carcinoma [1]. CRC is difficult to detect due to the insidious nature of symptoms [2] and in 2006 the bowel cancer-screening programme was introduced in the UK to try and improve survival by earlier diagnosis [2]. Despite this introduction, we continue to learn about this common and deadly disease and we are yet to see the drop in mortality of 16% that was predicted [2]. We present an unusual presentation of early CRC in a 68-year-old male.
Case Report
A previously fit and well 68-year-old male presented with a 6-month history of pain in the right hip. On examination this was localised to the superior area of the hip joint where a bony mass could be palpated. A pelvic radiograph was performed (Fig. 1) showing a bony exostosis on the right iliac wing. To characterise the lesion further, a pelvic Magnetic resonance imaging (MRI) scan was performed (Fig. 2). Appearances were consistent with an osteosarcoma and referral to the local sarcoma centre for histological investigation was made. Surprisingly, sampling from biopsy showed invasive well-differentiated adenocarcinoma. Staging computed tomography (CT) scanning did not reveal a primary source for the tumour but did identify thickening of the descending colon (Fig. 3) and lymphadenopathy involving the left supraclavicular, thoracic, paravertebral, retro-crurual and right inguinal regions. There was no evidence of tumour in the liver, lung or other parts of the skeleton. Subsequently, colonoscopy identified the thickened lesion as a hepatic flexure adenocarcinoma (Fig. 4). Biopsy at the time of endoscopy revealed the lesion at the hip to be a metastasis.

Radiograph demonstrating a right-sided iliac exostosis.
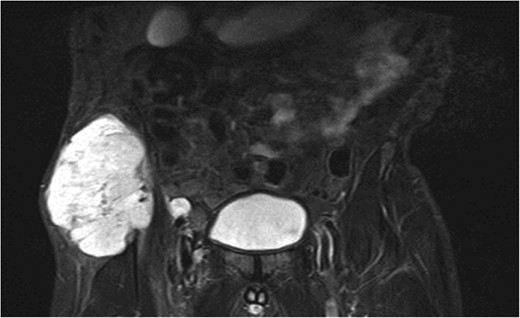
MRI showing a right-sided tumour involving the iliac wing.
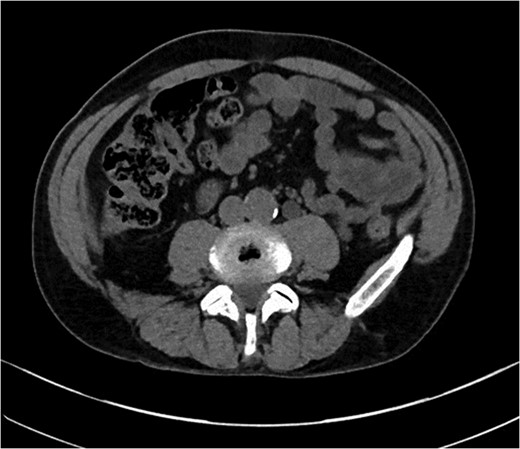
CT abdomen demonstrating thickened segment of ascending colon.
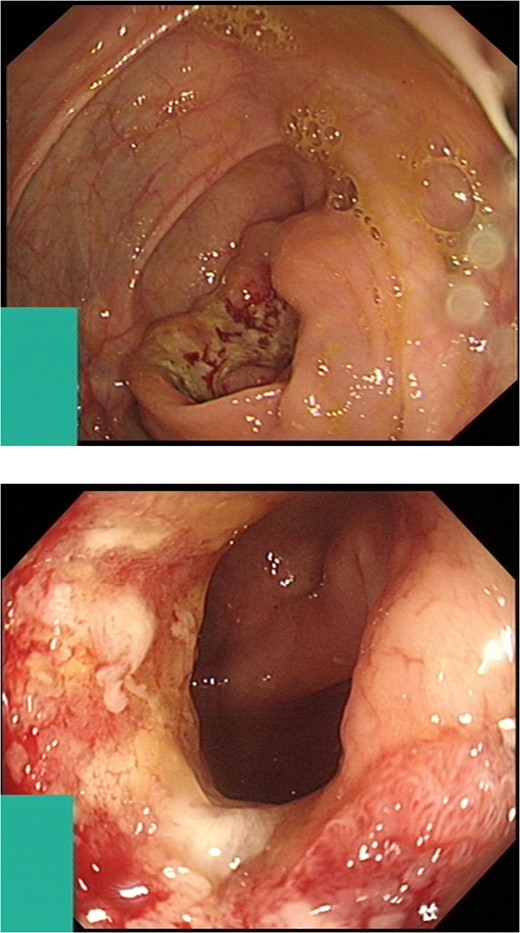
Intraluminal images demonstrating a lesion at the hepatic flexure.
Discussion
We present a rare case of colorectal adenocarcinoma mimicking osteosarcoma and presenting as hip pain at initial consultation. Early CRC is notoriously difficult to diagnose. Hamilton et al. [3]. performed a case-control study of 349 CRC sufferers and 1744 controls in primary care. Their results suggest that rectal bleeding, weight loss and abdominal pain were the three symptoms most strongly associated with CRC before diagnosis (Positive predictive values were 2.4, 1.4 and 1.2% respectively) [3]. Combined with a recent study suggesting only 5.5% of patients have bony metastasis at diagnosis [4] and the majority of these lesions (65%) are within the spinal column the presentation of our patient is novel. Further intrigue comes from the apparent identification of our patients’ bony metastasis in isolation. Roth et al. [5] performed a retrospective analysis of 252 CRC patients’ CT and PET CT reports and found that ‘metastasis only to bone without other organ involvement in colorectal cancer patients is extremely rare’ [5]. In fact, in their cohort of 252 patients, no patient had an isolated metastasis to bone.
In 2006 a national screening programme for CRC was introduced with the primary aim of early diagnosis and treatment. However, 47.75% of patients who received screening faecal occult blood tests did not return them [2]. Although this was expected from the previously performed pilot study [6], it is likely that as clinicians we will continue to see patients presenting for the first time in the advanced stages of CRC. As an example, our patient presented to orthopaedic services from primary care and although extremely unusual in the initial presenting complaint, showed signs of nodal disease with a large solitary metastasis of unknown origin. Our case demonstrates the vital role that histological sampling plays in the diagnosis and treatment of carcinomatous disease. It also demonstrates the need to maintain high index of clinical suspicion, no matter how benign the presenting complaint may seem.
Acknowledgements
The authors would like to acknowledge the Royal National Orthoapedic Hospital for their help in performing the biopsy and the preliminary histological analysis.
Conflict of Interest Statement
None declared.
Funding
There were no funding sources.

{kind=link}
{kind=link}
{kind=link}
{kind=link}