





Abstract
Bleeding from a caecal mass is a common clinical scenario encountered in surgical practice. Tumours, diverticulitis, inflammation and vascular malformations are the most common causes of this bleeding. We present a case of a submucosal bleeding caecal mass, which turned out to be an appendiceal faecolith protruding into the caecum. Although we found one reported case of this previously, it was not encountered in the emergency setting.
INTRODUCTION
Caecal faecolith is a very rare cause of a caecal lesion and iron-deficiency anaemia. The case reported here is presented to show the difficulties in accurate diagnosis and proper management.
CASE REPORT
A 72-year-old female presented to the Emergency Department with symptomatic anaemia. Past medical history includes atrial fibrillation and a stroke 6 months prior with no residual deficit. She was on apixaban (factor 10 inhibitor). She had noticed 3 months of progressive shortness of breath and tiredness. Her haemoglobin was 66 g/L in emergency. Iron studies showed Fe 3.2 mmol/L, transferrin 5.1 mg/dL, ferritin 159 pmol/L and iron saturation 27%, indicating iron-deficiency anaemia. She was admitted, transfused 2 units of red cells and had a diagnostic colonoscopy on Day 4 of her admission.
Shown in Fig. 1 is a colonoscopy view of the caecum showing the submucosal mass protruding into the lumen with a central ulceration and some slight ooze bleeding on biopsy.
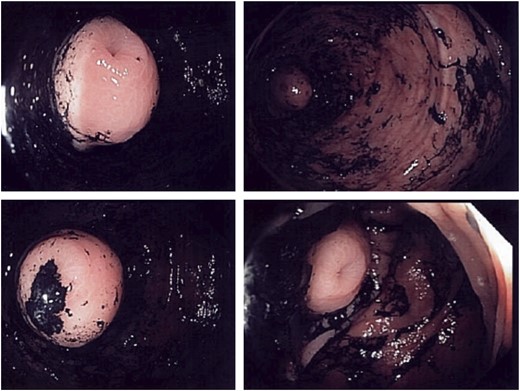
Colonoscopy views of the caecum.
On colonoscopy, she was found to have a caecal submucosal mass that bled when biopsy was attempted. It was 2–3 cm and appeared likely to be a gastrointestinal stromal tumor (GIST). Otherwise, the colonoscopy was normal.
CT abdomen was performed showing a 3 cm caecal mass likely submucosal; the histopathology of the biopsy taken on colonoscopy showed only normal colonic mucosa.
Shown in Fig. 2 is a CT scan showing the caecal mass near to the ileocaecal valve.

CT scan showing the caecal mass near to the ileocaecal valve.
Over the next few days, her haemoglobin slowly decreased and she had ongoing malaena requiring one more unit of transfusion. Surgical opinion was obtained for management of a likely bleeding GIST in her caecum. The decision was made for surgical resection rather than repeat colonoscopy or further imaging given the ongoing bleeding and likely diagnosis. She underwent a laparoscopic converted to open limited right hemicolectomy as the mass was close to the ileocaecal valve, so cecectomy was unable to be performed. Her recovery was complicated by some previously unknown heart failure and fluid overload, but this was settled on low-dose frusemide. She was discharged home on Day 7 postoperatively. Formal histopathology showed an appendiceal faecolith protruding back into the caecum underneath the submucosa resembling a mass
Shown in Fig. 3 is a macroscopic view of the resected specimen having been opened coronally, showing the faecolith in the obliterated appendiceal lumen and protruding back into the caecum.

A macroscopic view of the resected specimen.
DISCUSSION
Caecal lesions are a common cause of iron-deficiency anaemia and lower gastrointestinal bleeding. Colonoscopy is widely considered the gold standard for investigation and diagnosis of these lesions [1]. Submucosal colonic lesions usually appear as broad-based lesions protruding into the lumen with normal overlying colonic mucosa or ulceration. These lesions often appear to be extrinsic to the bowel lumen causing indentation. While there are many recognized causes of a colonic submucosal lesion being both benign and neoplastic [2], appendiceal faecolith presenting as a caecal mass is a rare cause having only previously been published once. In that previous case, the patient was not managed in the acute emergency surgical care setting and the diagnosis was made preoperatively [3]. Appendiceal faecoliths are a common finding in patients with acute appendicitis and also in normal appendices removed during diagnostic laparoscopies [4, 5]; however, these faecoliths remain confined to the appendiceal lumen. On detailed examination of the endoscopy pictures, there is a suggestion of the appendiceal orifice in the centre of the lesion, and this was endoscopically thought to be ulceration. This cases raises questions around preoperative investigation of uncommon colonic findings including CT colonography.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}