





Abstract
Associated tumors of the ovary and the appendix are commonly found in cases of pseudomyxoma peritonei (PP); the origin of these tumors are a continually debated topic. Outside of the setting of PP, this finding is exceedingly rare and there are no documented reports of two primary processes causing carcinomatosis in the absence of PP. Here, we present a patient who underwent cytoreductive surgery for peritoneal carcinomatosis presumptively secondary to ovarian carcinoma and who on pathological examination was found to have synchronous primary malignant processes of both the appendix and the ovary. This represents the first documented case of carcinomatosis resulting from two separate malignant processes in the absence of PP.
INTRODUCTION
Peritoneal carcinomatosis most often occurs as a result of metastatic spread of a prior-existing tumor of the abdomen or pelvis, most commonly colorectal cancer, ovarian cancer, appendiceal cancer, stomach cancer and pancreatic cancer; rarely, peritoneal carcinomatosis can occur as a primary malignant disease process of the peritoneum. In women, associated tumors of the ovary and the appendix are commonly found in cases of pseudomyxoma peritonei (PP), with the origin of these tumors being a continually debated topic [1, 2]. Outside of the setting of PP, however, there are only two documented reports of independent synchronous tumors of the ovary and appendix [3, 4], and no reports of two primary processes causing carcinomatosis in the absence of PP. Here, we present a case where a patient with invasive peritoneal carcinomatosis was found to have synchronous primary malignant processes of the appendix and the ovary.
CASE REPORT
A 51-year-old female with a past medical history significant only for hysterectomy and right oophorectomy for fibroid disease presents to the emergency department complaining of diffuse abdominal pain and increasing distention. A computed tomographic scan of the abdomen and pelvis demonstrated bilateral adnexal masses, extensive omental caking and prior hysterectomy. Additionally, tumor markers, cancer antigen-125 and carcinoembryonic antigen (CEA) were elevated to 196 U/ml and 14.5 ng/ml, respectively. A chest X-ray was negative for evidence of pulmonary metastasis and a colonoscopy did not reveal colonic tumor.
With a presumed diagnosis of ovarian cancer with carcinomatosis, the patient was presented with a treatment plan including cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (HIPEC); after lengthy discussion, the patient agreed to go forward with the procedure. On laparotomy in addition to extensive carcinomatosis, the patient was found to have a right sided malignant-appearing retroperitoneal process involving the appendix, cecum and right colon as well as a separate different appearing left-sided process involving the left ovary and sigmoid colon. Cytoreductive surgery included en bloc resection of right retroperitoneal mass involving the appendix and cecum, total colectomy, proximal protectomy, left oophorectomy en bloc with partial small bowel and partial bladder resection, total peritonectomy and cholecystectomy. The patient then underwent HIPEC for 90 minutes with mitomycin C at 10 mg/m2. Following HIPEC, an ileorectal anastomosis with loop ileostomy was performed and a central venous catheter with access port was placed in anticipation of future chemotherapeutic treatment. The patient was extubated and transferred to the ICU for further care with normal postoperative recovery with discharge on postoperative day 12.
Subsequent surgical pathology results confirmed two separate malignant processes causing the carcinomatosis: Immunohistochemical examination was performed on the surgical specimens. The appendiceal tumor stained negative for CK-7 and positive for CK-20 (Fig. 1), whereas the ovarian sample stained positive for CK-7 and negative for CK-20 (Fig. 2), consistent with malignant processes of independent origins.
Perforated mucinous adenocarcinoma of the appendix arising from villous adenoma, at least 8.5 cm invading into subserosa and into adjacent ileal and cecal serosa with widespread involvement of omentum (carcinomatosis).
Left perforated ovarian mucinous adenocarcinoma with widespread involvement of fallopian tube and subserosa of sigmoid colon (carcinomatosis).
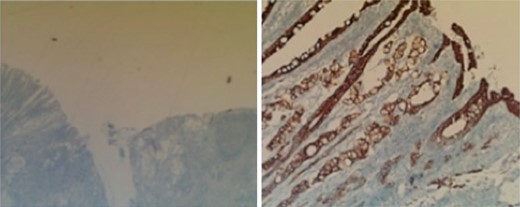
Appendix. CK-7 stain (left) and CK-20 stain (right).
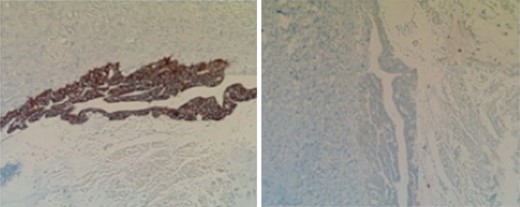
Ovary. CK-7 stain (left) and CK-20 stain (right).
DISCUSSION
In the available literature, synchronous tumors of the ovary and appendix are an uncommon yet well-recognized occurrence in the setting of PP. The origin of such synchronous tumors is widely debated with most evidence favoring a primary appendiceal tumor with the ovarian tumor representing a metastatic process [1, 2].
To address the questions of tumor origin in PP, Ronnett et al. [5] studied a series of 68 women with PP, 30 of which had ovarian involvement, and found that none of these cases were unequivocally ovarian in origin. As is the case with this example, existing literature on coexisting appendiceal and ovarian tumors resulting peritoneal dissemination by malignant processes is limited to those presenting with the less grave process of PP.
In the absence of PP, there have been only two cases, to our knowledge, of synchronous tumors or the ovary and appendix with each representing a primary process as reported by Rudzki et al. [3] and Bozanovic et al. [4]. In Rudzki's case, the appendix appeared grossly normal and appendectomy was performed as routine in the setting of total abdominal hysterectomy with oophorectomy for large right-sided ovarian tumor. Investigation with immunohistochemical staining revealed a CK7+ and CK20− phenotype of the ovarian tumor and the opposite (CK7− and CK20+) in the appendiceal tumor. This is proposed as evidence for independent primary processes. Bozanovic et al. present a patient found to have a mass of the cecum with adhesion to the right ovary on exploratory laparotomy for acute abdomen; subsequent pathology revealed serous papillary carcinoma of the ovary and adenocarcinoma of the appendix.
In the case we present here, gross intraoperative inspection demonstrated carcinomatosis in the absence of PP with appendiceal and left-sided ovarian processes that were not adhered to one another, and each seeming to have ruptured separately with apparently distinct surrounding processes. Immunohistochemical examination also revealed these opposing phenotypes of CK7+ and CK20− in the ovarian tumor and CK7− and CK20+ in the appendiceal tumor just as had been the case in the Rudzki's case as mentioned above. In our current literature search, this is the first report of two primary synchronous tumors resulting in carcinomatosis in the absence of PP.
To summarize, association of mucinous tumors of the appendix and ovary is a well-recognized entity, but recognition as synchronous primary processes is still widely debated. In any event, the vast majority of these associated cases are documented in the setting of PP with only two cases being documented in the absence of this finding. Here, we have presented a compelling not yet reported case of synchronous primary malignant tumors of the ovary and appendix, as evidenced by their opposing immunohistochemical phenotypes, causing carcinomatosis in a single patient in the absence of PP.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}