





Abstract
Humerus fracture is very rarely associated with ipsilateral shoulder dislocation. Here, we have reported probably the first case of compound fracture of humerus associated with a two-part fracture dislocation of ipsilateral shoulder. A 30-year-old female presented to the emergency department after a road traffic accident. The vehicle in which she was travelling skidded off the road and she got trapped. She had degloving injury over her left arm with a fracture of left humerus and anterior dislocation of ipsilateral shoulder and greater tuberosity fracture. She was managed initially with wound debridement, external fixation over humerus, closed reduction of shoulder dislocation, and open reduction and internal fixation of greater tuberosity fracture. Skin grafting was done over the wound later on. Fracture united at 4 months with a good range of movement at shoulder at the final follow-up.
INTRODUCTION
A combination of fracture shaft of humerus with ipsilateral shoulder fracture dislocation is rare injury. Only few cases are reported in the English literature till date having anterior dislocation of shoulder and ipsilateral closed humeral shaft fracture [1–10]. There are cases of two-part fracture dislocation associated with humeral shaft fracture [2, 5–8, 10] and cases of three-part fracture dislocation associated with humeral shaft fracture [9]. There is no consensus regarding management and mechanism of injury.
We report an even rarer combination of injury where there was a two-part fracture dislocation of shoulder and ipsilateral compound fracture of humerus shaft. We have discussed the probable mechanism of injury, and share our difficulties while managing this case and have reviewed the literature.
CASE REPORT
A 30-year-old female came to the emergency department at midnight following a road traffic accident with severe pain and swelling over the left shoulder and arm. Her arm was trapped when the vehicle in which she was travelling skidded off the road. On examination she had degloving injury over posteromedial aspect of the arm extending to axilla with acute bend over arm and loss of shoulder contour (Fig. 1A). Her distal neurovascular structures were intact. Axillary nerve was intact. X-ray (Fig. 1B) showed anterior dislocation with displaced greater tuberosity fracture and transverse fracture of humerus in its middle third. She was managed on next morning. Wound was debrided thoroughly and washed adequately with normal saline. An external fixator was applied on humerus and then shoulder was reduced without difficulty. After reduction, greater tuberosity fracture was found displaced so it was fixed with a cannulated cancellous screw through a deltoid splitting approach (Fig. 1C). Skin grafting over the raw area was done on 10th day after the wound bed was ready. There was poor take over axillary region so another grafting was done after 1 week. After 3 weeks, wound healed completely and then, passive movement at shoulder joint was started. After two and half months, the external fixator was removed and functional brace was applied. After 4 months, the fracture had united completely (Fig. 1D) and brace was discontinued. She had a useful range of motion at the time of brace removal, with abduction and flexion of around 90°. External rotation was ∼20° while internal rotation was normal. At the last follow-up of 11 months, she had a good range of motion with abduction and flexion of 160°flexion and full rotation.
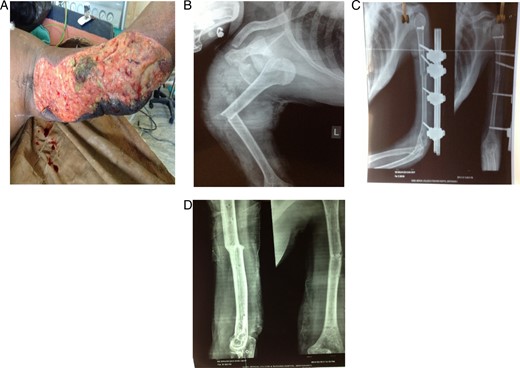
(A) Clinical picture at the time of presentation to emergency. (B) Preoperative X-ray of left shoulder with arm anteroposterior view showing dislocation of shoulder, greater tuberosity fracture and humerus mid-shaft fracture. (C) Postoperative X-ray showing shoulder reduction, greater tuberosity fracture fixation with a cannnulated screw and humerus fracture fixed with external fixation. (D) Four months postoperative X-ray showing fracture union.
DISCUSSION
Fracture shaft of humerus associated with ipsilateral dislocation is rare injury, whereas isolated shoulder dislocation or humerus fracture is very common. The first such case was reported by Winderman [1] in 1940. Anterior dislocation is relatively more common than posterior, in association with humerus shaft fracture. Of the reported cases, almost all have closed shaft fracture. So, this case, where we have the fracture dislocation with ipsilateral compound fracture of humerus shaft, is probably one of the few reported cases and is important due to three aspects.
The first aspect is the mechanism of injury. Similar case reports in the literature have advocated two possible mechanisms of injury. Sankaran-Kutty and Sadat-Ali [6] suggested that force exerted along the axis of the humerus simultaneously fractured the humerus and dislocated the shoulder, whereas Kontakis et al. [4] proposed that the shoulder dislocated first and subsequent, bending or torsion forces fractured the shaft of humerus. We believe that the mechanism of injury in our patient was as described in the second case by Kontakis et al. [4], and this is supported by the fracture pattern that is transverse, acute bending of arm during emergency presentation and degloving of skin flap over arm with compounding of fracture.
The second important aspect of our case is its management. There is no consensus on the management in the reported cases till now. Almost all have reported closed reduction of shoulder. Closed reduction is sometimes assisted by Steinman pin as reported by Barquet et al. [10] and Winderman [1]. Sankaran-Kutty and Sadat-Ali [6] used limb lengthening apparatus to assist in closed reduction of shoulder. Open reduction was required in cases reported by Kontakis et al. [4] and Baker [2]. Only in few cases, the authors have reduced the shoulder prior to fracture fixation [7], otherwise all have fixed fracture before reduction of the shoulder. Authors differ in fracture management. Splint, casting [1, 3, 4, 9, 10], plates and screw [4, 5, 8], external fixator [6] and even intra-medullary nail [2, 3] all have been used with consistent result in fracture union. In our case too, we fixed the fracture prior to reduction. We were bound to use external fixator in our case due to compound nature of injury. We fixed the greater tuberosity fragment through a deltoid splitting approach after thorough debridement of wound and did skin grafting on the raw wound later. We believe that external fixator is not ideal for humerus fracture with shoulder dislocation as it is cumbersome, it affects mobilization and hence the outcome of shoulder movement but it has consistent results on fracture union. The presence of wound required skin grafting later and this also affected early mobilization of the shoulder.
The third aspect of this case is its outcome. Almost all reported cases have reported satisfactory outcome (some degree of restriction of abduction and flexion) despite different modalities of management. We also had a good outcome in our patient despite having more severe injury, open fracture and associated fracture of greater tuberosity and the fact that she was managed with external fixator initially. We believe that following the basic principles of trauma care was the key for good outcome in this case.
CONFLICT OF INTEREST STATEMENT
None declared.
ACKNOWLEDGEMENT
I thank Dr Manisha Chhetri for editing the manuscript.

{kind=link}