





Abstract
Laparoscopic subtotal cholecystectomy is a technique that is becoming increasingly prevalent in modern surgery. It avoids the cystic duct and artery where acute or chronic cholecystitis prevents a safe laparoscopic dissection of these structures. There are numerous reports of symptomatic cystic duct remnants after subtotal cholecystectomy in the literature on post-cholecystectomy syndrome. We present a case report of a 62-year-old man who underwent emergent laparoscopic subtotal cholecystectomy complicated by the development of a persistent, controlled bile leak. This was followed on serial ultrasound examinations and managed with multiple drain insertions and endoscopic retrograde cholangiopancreatography. The patient represented 4 months later with right upper quadrant pain and was found to have an apparently normal gallbladder on CT abdomen. Repeat laparoscopic cholecystectomy demonstrated a reformed gallbladder wall and was completed in the standard fashion. This case demonstrates an unexpected complication of laparoscopic cholecystectomy with correlation of radiological and surgical findings.
INTRODUCTION
Open subtotal cholecystectomy was first described in 1985 by Bornman and Terblanche [1]. The procedure was later adapted in 1993 to the laparoscopic technique [2, 3]. There are three described methods that may avoid dissection of the triangle of Calot. Type 1 involves transection at the neck of the gallbladder with no dissection or ligation of the cystic duct or artery and a sutured closure of the proximal stump. Type 2 leaves the hepatic aspect of the gallbladder wall intact. Type 3 involves a combination of the first two techniques [4, 5]. On completion of the subtotal cholecystectomy, regardless of the type, there is extensive cauterization of any residual gallbladder mucosa.
Subtotal cholecystectomy is primarily utilized in the setting of significant acute or chronic cholecystitis as it avoids potentially unsafe dissection and subsequent trauma to the biliary tree and adjacent structures.
Within the literature on the post-cholecystectomy syndrome, there are multiple articles and case reports documenting the presence of cystic duct remnants after subtotal cholecystectomy, some of which develop calculi [2, 6]. We present a case study of ‘reformed gallbladder’, wherein the gallbladder remnant after subtotal cholecystectomy has been followed with serial ultrasound examination. It formed a distinct compartment, which strongly resembles a normal gallbladder on interval CT scan, and required repeat laparoscopic cholecystectomy.
CASE REPORT
A 62-year-old man presented to the emergency department with 3 weeks of intermittent right upper quadrant pain. CT of the abdomen demonstrated acute cholecystitis complicated by a contained perforation of the gallbladder at the hepatic aspect. A Type 3 laparoscopic subtotal cholecystectomy was performed the day after his admission due to an inability to safely dissect inflammatory adhesions, which held the duodenum in close proximity to the structures of Calot's triangle. The remaining gallbladder tissue was diathermied and a drain was placed in the gallbladder fossa.
This patient remained in hospital for 1 month with postoperative complications. Ongoing leakage of bile prompted insertion of a percutaneous drain and endoscopic retrograde cholangiopancreatography with stent insertion. Ultrasound of the abdomen performed on Day 14 postoperatively demonstrated a collection with lobulated margins (Fig. 1). Concurrent hepatobiliary iminodiacetic acid scan confirmed that this represented an ongoing bile leak contained within the gallbladder fossa.
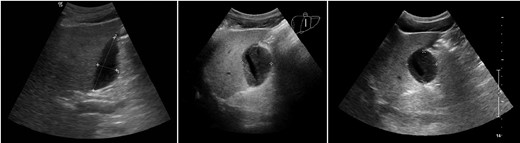
Ultrasound on postoperative Days 14 (left), 21 (middle) and 31 (right). Liver is on the left in each image, and the persistent collection is demonstrated within the gallbladder fossa.
Further ultrasound studies on Days 21 and 31 demonstrated an ongoing organizing collection (Fig. 1). He was discharged with the percutaneous drain in place, which was removed on Day 37 when drainage eventually ceased.
The patient presented to the hospital 4 months after the initial operation with right upper quadrant pain. CT abdomen established the appearance of a normal gallbladder despite his history of subtotal cholecystectomy (Fig. 2). He underwent an elective laparoscopic cholecystectomy 1 month later, which revealed an apparently complete gallbladder that was extensively walled off by omentum. An intraoperative image is shown in Fig. 3.
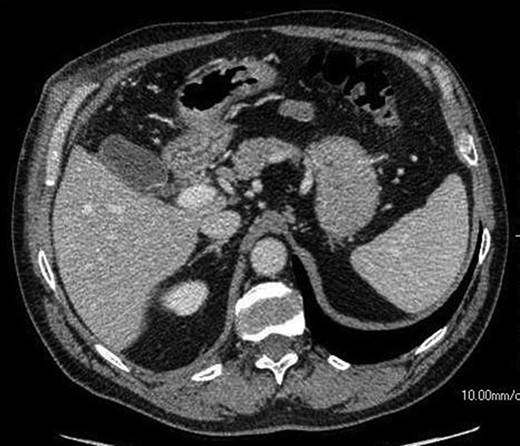
An axial CT image shows collection in the gall bladder fossa closely resembling a normal gallbladder appearance.
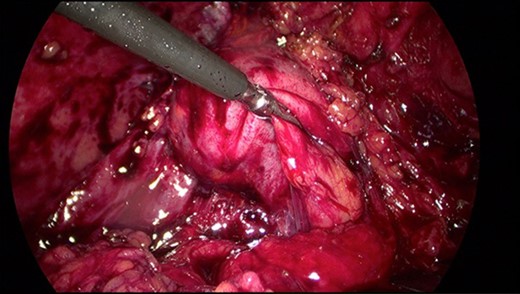
Intraoperative image of Hartmann's pouch (held by graspers) in continuity with a reformed gallbladder.
The postoperative recovery was uneventful and the patient remained pain and gallbladder free. Acute on chronic cholecystitis and contiguous gallbladder mucosa were demonstrated by histopathological analysis.
DISCUSSION
This study presents radiological correlation of an interesting surgical case. The progressive ultrasound images demonstrate organization and localization of a postoperative collection, which is later indistinguishable from normal biliary anatomy on CT. This finding is confirmed intraoperatively.
At present, there is little long-term data available documenting the rate of complications of subtotal cholecystectomy, and studies currently available are often of retrospective design and have small sample sizes [2]. As laparoscopic subtotal cholecystectomy increases in popularity (and open conversions subsequently decline), this case demonstrates potential for an unexpected postoperative outcome. Additionally, it highlights that further imaging may be quite useful in patients with recurrent symptoms following subtotal cholecystectomy.
CONFLICT OF INTEREST STATEMENT
None declared.
REFERENCES
Author notes
†To our knowledge, this is the first correlation of radiological and intraoperative findings in reformed gallbladder after subtotal cholecystectomy and we believe it would appeal to the readership of the Journal of Surgical Case Reports. This manuscript has not been published and is not currently submitted for review by any other journal or publishing body.

{kind=link}
{kind=link}
{kind=link}