





Abstract
Acquired external auditory canal atresia is a rare complication of chronic inflammatory otitis, and is generally fibrous or soft tissue in nature. Here, we present the first reported case of heterotopic ossification within chronic fibrosing otitis externa in a 25-year-old male patient with a childhood history of granular myringitis and failed tympanoplasty. A calcified mass was demonstrated adjacent to the tympanic membrane on CT imaging, and surgical exploration revealed a cohesive bar of bone traversing the medial external auditory canal. Drill canaloplasty and split-thickness skin graft coverage of the lateral tympanic membrane resulted in an improvement in the pure tone average from 79 to 55 dB. As the treatment for chronic fibrosing otitis externa involves the surgical widening of the external auditory canal, we alert surgeons to the possibility of cohesive bone formation as a potential cause of navigational confusion and inadvertent over- or under-drilling of the canal stenosis.
INTRODUCTION
Acquired canal atresia, which can rarely occur secondary to chronic inflammation, is generally fibrous or soft tissue in nature. Here, we present the first reported case of heterotopic ossification in postinflammatory obliterative otitis externa.
CASE REPORT
A 25-year-old man presented to our department with long-standing left-sided hearing loss. He underwent bilateral grommet insertion in childhood for recurrent otitis media complicated by a discharging left ear postoperatively. On grommet extrusion, he had a persistent left small central tympanic perforation with granulations, with subsequent unsuccessful fat graft myringoplasty at the age of 16. Conservative management witnessed spontaneous closure of the perforation, but with the development of a distorted appearance of the posterior tympanic membrane over the ensuing 7 years. He continued to have intermittent left otorrhoea throughout this period, but eventually achieved a dry ear with improvement of his pure tone audiogram threshold from a 40-dB conductive loss to 20 dB. He was discharged from otology at this point, but presented to our services 8 years later following deterioration in his left-sided hearing over the preceding year.
On assessment, he denied otorrhoea or other otological symptoms. His general medical history was unremarkable. His left tympanic membrane had a normal anterior appearance, but the posterior half of the external auditory canal was obliterated. His right ear was unremarkable, except for a patch of myringosclerosis. Audiometry revealed a right mild high tone sensorineural hearing loss (presumed secondary to previous otitis media) and a left severe mixed hearing loss (pure tone average 79 dB) associated with a type B tympanogram. CT imaging confirmed a normal middle ear cleft, with a plug of soft tissue containing dense calcification 8 mm lateral to the tympanic membrane (Fig. 1), consistent with a diagnosis of left chronic fibrosing otitis externa.
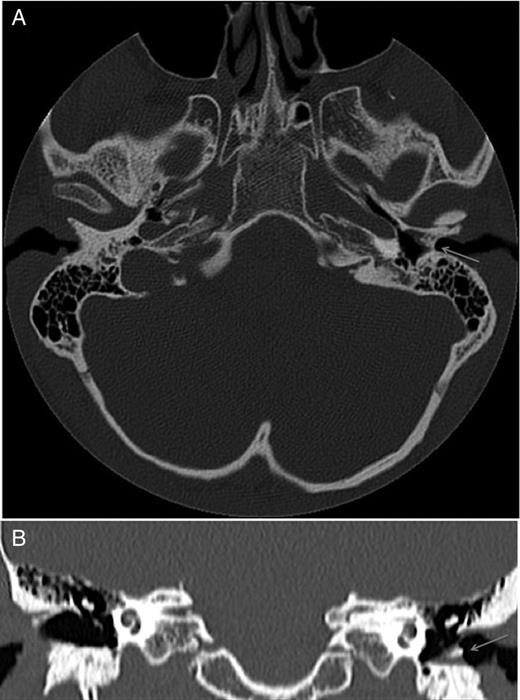
CT temporal bone axial (A) and coronal (B) slices, demonstrating a soft tissue thickening of the left medial external auditory canal containing dense calcification (arrow).
To improve his hearing, he underwent a left external auditory canaloplasty. At operation, the skin overlying and immediately lateral to the posterior tympanic membrane was thickened and fibrosed, confirming the radiological findings. A 4-mm smooth bar of bone was found to be traversing the deep external auditory canal immediately lateral to the inferior tympanic membrane (Fig. 2). The calibre of the external auditory canal was otherwise normal and symmetrical with that of the right ear. The bony bar was drilled away taking care not to damage the tympanic membrane. Upon peeling off the remaining mass of fibrosis, the underlying tympanic membrane was intact. A partial-thickness graft harvested from postauricular skin was used to cover the de-epithelialized tympanic membrane and exposed bone of the deep external auditory canal. Postoperative audiometry showed an improvement in conductive hearing with a pure tone average of 55 dB.
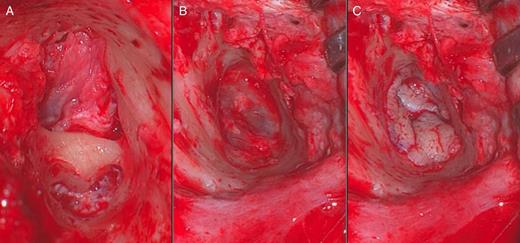
Intraoperative images showing the horizontal bony bar (A), view of an intact tympanic membrane post-drilling (B) and placement of a partial-thickness skin graft (C).
DISCUSSION
Postinflammatory chronic fibrosing otitis externa is a rare condition, with only a few case series reported in the literature. It is a form of acquired external auditory canal atresia characterized by fibrotic tissue causing obliteration of the medial external ear canal, usually following prolonged or repeated infection or inflammation in the presence of granulation tissue [1]. Typically, there is a long history of chronic or recurrent otorrhoea before the development of a dry ear with conductive hearing loss.
Heterotopic ossification is the formation of bone in soft tissues. It has been observed to occur in diverse tissue types [2] and is thought to result from osteoblast differentiation from the mesenchymal progenitor which secretes bone morphogenetic proteins [3]. Within the middle ear, heterotopic ossification can be seen in tympanosclerosis or, rarely, in myringosclerotic plaques [4].
This is, to our knowledge, the first reported case of cohesive bone formation in chronic fibrosing otitis externa. The consensus for surgical management for chronic fibrosing otitis externa is excision of all fibrotic tissue while preserving the fibrous layer of the tympanic membrane, and the use of skin flaps or grafts to cover bare bone [1]. Widening of the underlying bony canal may be necessary to enable excision, but the surgeon needs to be aware of the risk of damage to the facial nerve posteroinferiorly and the temporomandibular joint capsule anteriorly. Risk is minimized through the recognition of bony anatomical landmarks, perhaps augmented with facial nerve monitoring. We alert surgeons to the possibility of heterotopic ossification of the external auditory canal, as described here, as a potential cause of navigational confusion and inadvertent over- or under-drilling of canal stenosis.
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief on request.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}