





Abstract
Boerhaave syndrome is a spontaneous perforation of the oesophagus secondary to forceful emesis. Surgery has been advocated in delayed presentations of Boerhaave's syndrome with mediastinitis. The over-the-scope clip (OTSC) by OVESCO® (Tubingen, Germany) has been used in the endoscopic management of gastrointestinal bleeds, fistulae and anastamotic leaks. We describe the successful endoscopic use of the OTSC in a delayed presentation of Boerhaave syndrome with mediastinitis. A 69-year-old gentleman underwent a computerised tomography scan, which demonstrated a lower oesophageal perforation and mediastinitis 7 days after admission, having presented with forceful emesis and chest discomfort. During endoscopy the defect was visualized and successfully closed using the OTSC. This resulted in a favourable outcome and is a technique not previously described in the literature to manage this condition.
INTRODUCTION
Boerhaave's syndrome is a spontaneous longitudinal perforation of the oesophagus due to forceful emesis first described by Hermann Boerhaave in the 18th century [1]. The classic anatomical location for this is the distal third of the oesophagus. Mackler's triad of subxiphoid chest pain, vomiting and subcutaneous emphysema is present only in 14% of cases. Hence detection can prove a diagnostic challenge, but requires swift intervention to ensure a favourable outcome. The use of contrast swallow may aid diagnosis, but this has a false-negative rate of 10% and in such cases computerised tomography (CT) provides a good diagnostic tool [2].
Current evidence agrees that cases identified within 24 h of presentation should be managed with surgery. There is no ‘gold standard’ for the management of Boerhaave's after the acute phase of presentation. However, the condition may be managed conservatively in cases of a contained perforation. In those with mediastinal contamination, evidence has been in favour of surgery [3].
With recent advances in endoscopy, successful management of iatrogenic perforations have been described using stenting and clipping techniques.
There are few cases in the literature of endoscopic clipping being used for Boerhaave's syndrome [4, 5]. In this case report we describe the first case of a delayed presentation of Boerhaave's with mediastinal contamination managed by an over-the-scope clip (OTSC)®.
The OTSC designed by OVESCO® (Tubingen, Germany) has been described in a number of publications. The OTSC clip for flexible endoscopy is a super elastic Nitinol device for compression and approximation of tissues. The OTSC clip is delivered by means of an applicator cap mounted to the tip of gastroscopes or colonoscopies [6]. Its use has been demonstrated for management of gastrointestinal (GI) bleeds, fistulae, anastamotic leaks and perforations. However, it is yet to be described as an endoscopic measure to manage Boerhaave's syndrome.
CASE REPORT
A 69-year-old gentleman presented to hospital following an episode of forceful vomiting and chest discomfort. An initial chest radiograph revealed a left-sided pleural effusion. After several days with no improvement in the patient's condition, it was decided to perform a CT chest, which showed a suspected oesophageal perforation with mediastinitis. Two water-soluble contrast swallows were performed, which showed no leak and thus it was decided to continue to treat the patient conservatively.
However, a subsequent contrast CT scan showed a persistence of the perforation with ongoing mediastinitis (Fig. 1). In consideration of the size of the defect and the delay in presentation, it was decided not to perform surgery. An endoscopy revealed a persistent perforation at the lower oesophagus. This was closed successfully using the OTSC. This is demonstrated by a subsequent contrast swallow, showing no leak of contrast with the clip in place (Fig. 2). A naso-jejunal tube was inserted at the same time to facilitate post-pyloric feeding. The patient was initially managed with total parenteral nutrition post procedure for 3 days before being fed via an NJ tube. Furthermore, the patient was treated with intravenous antibiotics and bilateral chest drains were inserted. These measures resulted in a successful closure of the defect and resolving mediastinitis. The patient was later discharged from hospital with no further complications. At 6-month follow up, he was clinically well apart from a left-sided small chronic empyema, which was drained.
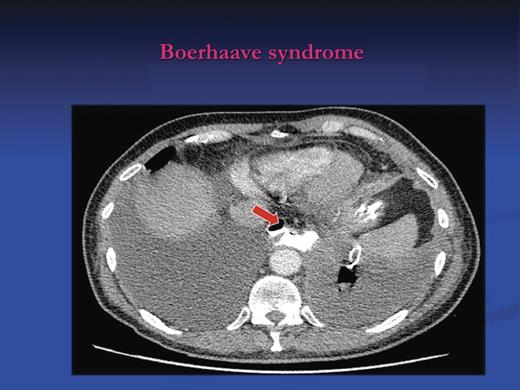
CT scan demonstrating left intercostal drain in situ. There is a tear in the distal third of the oesophagus on the left posterolateral aspect. Contrast has extravasated to fill a cavity in the posterior mediastinum ∼3.9 × 2.5 cm at its widest point in the axial plane and ∼10.5 cm in craniocaudal extent.

Contrast swallow after the application of the OTSC. Contrast passed beyond the distal oesophageal staples into the stomach and the duodenum; no contrast leakage is demonstrated.
DISCUSSION
Management of delayed oesophageal perforations after 24 h of presentation is a topic that needs further evaluation.
We have described the first case of sub-acute Boerhaave's syndrome with mediastinitis to be managed with endoscopic clipping using the OTSC clip. Current guidance would have advocated the use of surgery in this case. We have shown a favourable outcome without the need for this.
Endoscopic clipping has been advocated in <1.5 cm clean perforations with minimal signs of infection. Its use has been reported within the first 24 h of presentation of Boerhaave's syndrome. Three case reports have detailed endoscopic clipping in delayed presentations of Boerhaave's syndrome. Matsuda et al. [4] described clipping in a patient with no evidence of mediastinal contamination. Siriam et al. [5] used endoscopic clipping in a patient with sepsis and bilateral pneumothoracies.
One case report in the literature has shown the use of endoscopic clipping in a patient with a mature oesophageal perforation with mediastinitis. This was in a patient with a perforation secondary to foreign body ingestion and not Boerhaave's as in this case [7].
In this case, we have used the new over-the-scope clip, which has the advantage of closing larger defects without the chances of migration as in cases through the scope endoclips.
Kirchniak et al. [8] described the successful use of OTSC clip in 50 patients for haemostasis, closure of gastric perforations and fistulae. Sandmann et al. [9] described a series where defects within the digestive tract could be closed in 9 of 10 cases by the OTSC system®: fistulas (oesophagotracheal, oesophagopleural, gastrocutaneous and colovesical), perforations (after mucosectomy, after papillotomy and percutaneous endoscopic gastrostomy misplacement) and anastomosal leakages. A further study describes the use of the OTSC in eight patients with GI perforations. Three had colonic perforations, one with a perforation of the stomach and three with anastomotic leakage after gastrointestinal surgery [10].
Surgery has been the mainstay of management for delayed presentations of Boerhaave's syndrome with evidence of mediastinal contamination. However, advances in endoscopy can be used, as in this case, to manage such patients without the need for surgery. The main limitation being the size of the defect and degree of mediastinal contamination involved. Further studies and guidance are required in the management in delayed presentations and scenarios where minimally invasive techniques such as endoscopy may be indicated.

{kind=link}
{kind=link}
{kind=link}