





Abstract
The differential diagnosis of right lower quadrant abdominal pain includes both ureterolithiasis and acute appendicitis. Surgical treatment can be undergone without confirmatory imaging studies after a clinical diagnosis is made. For this reason, an occult, second abdominal process may be present.
A 47-year-old male presented with a three-day history of acute right lower quadrant abdominal pain. A contrast CT revealed both a 6 mm calculus obstructing the right ureter and acute appendicitis. The patient underwent appendectomy and ureteroscopy with stent placement at the same time.
Simultaneous appendicitis and ureterolithiasis may present with similar clinical findings. Due to the potential risks associated with missing either diagnosis, imaging studies may be an appropriate as a step in the management of the patient with right lower quadrant pain.
INTRODUCTION
Acute appendicitis typically presents as an isolated disease process with no other comorbidities. Acute renal colic caused by an obstructive ureterolithiasis is in itself usually a solitary finding. We present a case of a 47-year-old male who presented with acute right lower quadrant pain and associated symptoms suggestive of both renal colic and acute appendicitis.
CASE REPORT
A 47-year-old Caucasian male with two previous isolated episodes of nephrolithiasis presented with a three day history of non-specific umbilical abdominal pain, migrating to the right iliac fossa with radiation to the right back. His pain worsened upon movement. He reported decreased appetite over this period. He stated having similar episodes two months and three years prior; each time he was diagnosed with nephrolithiasis and required lithotripsy. Otherwise, he reported normal bowel movements and urinary habits without nausea, vomiting, fever, chills, or sweats.

CT showing thickened appendix
On physical exam the patient was afebrile (97.2F) with a normal pulse and blood pressure. An abdominal exam revealed right lower quadrant tenderness at McBurney’s point with no rebound or guarding and a negative Rovsing’s sign. Laboratory results revealed a white blood cell count of 10.3 x 109/L with a left shift, a BUN of 31 mg/dL, and a creatinine of 1.9 mg/dL. LFT’s and electrolytes were unremarkable.
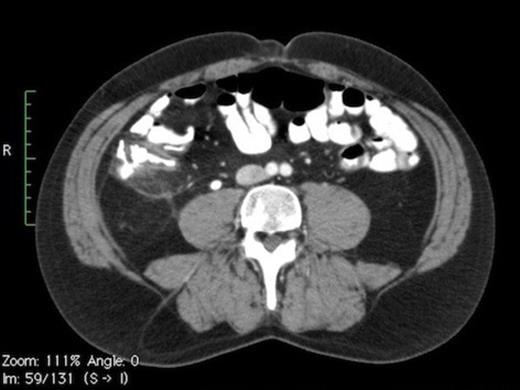
CT scan showing calculus in right mid-ureter
Contrast CT (Fig. 1A) depicts a thickened appendix measuring >12mm with periappendiceal fluid suggestive of acute appendicitis. Moderate hydronephrosis (Fig. 1C) of right kidney was noted with a 6mm calculus (Fig. 1B) in the right mid ureter.

CT scan showing moderate hydronephrosis
The patient elected to undergo right ureteral stent placement and laproscopic appendectomy. Both of which were preformed without complications.
DISCUSSION
Clinical findings remain a reliable and accurate method of diagnosing acute appendicitis (1). However some patients can present in an unusual way. Therefore several clinical prediction rules have been proposed to diagnose acute appendicitis(2-4). The Alvarado scoring system is one of such clinical diagnostic modalities to avoid the use of CT when deciding to proceed to appendectomy in such patients. However even with the use of scoring systems, the confusing picture that acute appendicitis can present at leads the clinician to choose computerized tomography for diagnosis. CT provides a higher sensitivity and specificity in diagnosis of acute appendicitis (5,6) and aids in the diagnosis of a concurrent disease process, as we have demonstrated in this case report.
The Overall lifetime risk of developing acute appendicitis in the United States is 8.6% and 6.7% for males and females respectively (7). The lifetime risk of developing urolithiasis is 10% and 5% for males and females respectively within the United States (8). Generally, acute appendicitis and renal colic present as separate processes. We present a case where the two acute processes occur together, and are distinguished prior to surgical intervention by the use of CT.

{kind=link}
{kind=link}
{kind=link}