





Abstract
Ectopic splenic tissue can present as accessory spleens and splenosis. While accessory spleens are congenital and more common; splenosis occurs as a result of implantation of splenic tissue as a result of trauma or iatrogenic injury. Only up to 40 intrathoracic splenosis have been reported in the English language literature to date. Here we discuss a case in which Para oesophageal pre-aortic ectopic splenic tissue was identified through radionuclide imaging 20 years after splenic rupture in a 44-year-old male for work up of epigastric pain.
Splenosis should be considered as differential diagnosis in all previously splenectomised patients who present with unexplained masses on imaging. Early diagnoses with preoperative non-invasive radionucleotide scanning with collateral histories can prevent unnecessary surgery and reduce expensive and invasive investigations.
INTRODUCTION
Ectopic splenic tissue can manifest in two distinct forms: splenosis and accessory spleens. Present in approximately 10% of the population, accessory spleens arise from the fusion failure of the splenic anlage and reside in close proximity to the splenocolic and gastrosplenic ligaments. (1) In contrast to this, splenosis is an acquired condition whereby splenic trauma or iatrogenic rupture can result in the autoplastic transplantation and implantation of splenic pulp throughout the containing cavity (2).
Intrathoracic implantation can arise as a sequel of splenic and diaphragmatic injury. Thoracic splenosis is an uncommon manifestation and, to date less than 40 cases have been documented in literature (3). Here we discuss a case in which Paraoesophageal pre-aortic ectopic splenic tissue was identified through radionuclide imaging 20 years after splenic rupture in a 44 year old male.
CASE REPORT
A 44 year old Caucasian male presented with a 9 year history of epigastric pain radiating to the back and associated with intermittent loose stool with worsening of symptoms in the preceding 18 months. His past medical history included diverticular disease, controlled hypertension, recurrent urethral strictures and a splenectomy 20 years previously following a road traffic accident (RTA).
Stool cultures, a coeliac screen and gastroscopy were normal. Flexible sigmoidoscopy and barium enema revealed diverticular disease within the left colon.
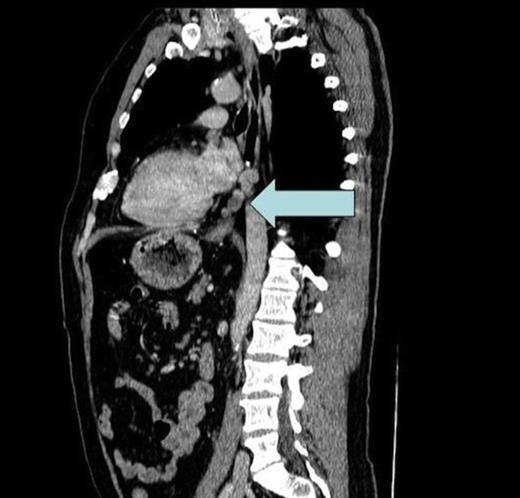
CT scan showing enlarged soft tissue deposits in a left paraoesophageal, pre-aortic site within the posterior inferior mediastinum
Suspecting occult pancreatic pathology a computerised tomography (CT) of the chest, abdomen and pelvis was performed. There was occult fibrosis post splenectomy and mild anatomical distortion at the tail of the pancreas and left diaphragm. However, the scan also identified enlarged soft tissue deposits in a left paraoesophageal, pre-aortic site within the posterior, inferior mediastinum (level of D8-D10); the largest deposit measuring 18mm in diameter (Fig. 1). Structures normally residing here are predominantly lymph nodes and at this size would suggest pathological enlargement.
Taking into consideration the patient’s splenectomy the possibility of ectopic splenic tissue was entertained and a radionuclide pertechnetate liver-spleen scan was organised. Planar and SPECT images were acquired of the chest and upper abdomen. Foci of increased tracer uptake were seen in Paraoesophageal and para-aortic regions that corresponded to the soft tissue masses seen on CT.
DISCUSSION
Following splenic trauma or iatrogenic rupture, splenic pulp is implanted onto surfaces within the exposed anatomical compartment. Although a portion of the tissue undergoes necrosis at the implantation site, it has been seen in animal models that small arteries and peri-arterial sheaths evolve and support the splenic tissue enabling regeneration (4).
In the majority of cases splenosis is confined to the anatomical limitations of the abdominal and pelvic cavities. (2) Cases of thoracic splenosis remain rare with at the time of writing less than 40 documented cases being recorded in literature (3). Mostly these follow concomitant rupture of the spleen and left hemidiaphragm (5). Only 10 cases of intrathoracic splenosis have been reported literature where a diagnosis has been achieved nonoperativly (5-7)
Owing to the higher incidence of splenic injury involving young males the male-to-female ratio is 30:8 (8).
Symptoms arising from thoracic splenosis are rare and majority of them are discovered incidentally on imaging (9). In the few cases that do exhibit symptoms they are predominantly confined to pleurisy and haemoptysis (8).
Splenosis may mimic lymphadenopathy, which commonly leads to extensive investigation for malignancy (2). The absence of spleen raised the possibility that these represented ectopic splenic tissue. Non-invasive investigation through radionucleotide scanning is the gold standard of testing in patients that have suspected ectopic splenosis (10). By demonstrating uptake of 99m-Tc sulphur colloid or 99m-Tc-labelled heat-denatured erythrocytes within the splenules a diagnosis can confidently be made (10).
Splenosis is predominantly identified as an incidental finding on imaging. As ectopic splenic tissue closely mimics lymphadenopathy extensive investigation to exclude malignancy are not uncommon. Early diagnoses with preoperative non-invasive radionucleotide scanning of patients with collateral histories can prevent unnecessary surgery and reduce expensive and somewhat invasive investigations. Splenosis is a differential diagnosis that should be considered in all previously splenectomised patients who present with unexplained masses on imaging.

{kind=link}