





Abstract
Gynaecomastia is a common examination finding in adult men. Supernumery breasts along the milk line are also identified frequently in the adult population. Here we report a case of ectopic gynaecomastia, away from the milk line. A 28-year-old man with no other health problems attended the general surgical clinic with a lump on the inner aspect of his left leg. This was thought to be a lipoma by the referring General Practitioner. It was however noted to have an associated nipple areolar complex and ultrasound confirmed mixed density breast tissue with no evidence of malignancy. Excision was undertaken and histopathology confirmed this to be breast tissue. In this case report, we report the first case of ectopic gynaecomastia in this region in an otherwise healthy man.
INTRODUCTION
Enlarged breast tissue in the male patient, gynaecomastia, is a common clinical examination finding. It can be physiological, iatrogenic or as a result of neoplastic processes [1].
Ectopic breast tissue in female patients is also a common finding on examination. Supernumerary breasts with or without associated nipple areolar complexes can be found from the axilla to the inguinal region. Accessory breast tissue out-with this embryological milk line is, however, less common [2, 3]. To the extent of our review, there have been no previous reports in the literature of gynaecomastia development in an accessory breast out-with the embryological milk line.
The following case report is of a man who developed accessory gynaecomastia in the inner aspect of his upper thigh.
CASE REPORT
A 28-year-old man attended the general surgical outpatient clinic with a mass in the upper medial aspect of his left thigh. This had been thought to be a lipoma by his General Practitioner and was referred for consideration of its removal. The patient was otherwise healthy and denied any pain, infection or discharge from the lesion over the preceding years. The lump was present since puberty and was slowly enlarging in size to the extent that it had started interfering with his gait on walking or running and it was these symptoms that led him to present for medical attention.
On examination, a 10 × 5 cm lesion was identified in the medial aspect of his left upper thigh. This was discrete from genitalia and was associated with a nipple areolar complex (Fig. 1 and 2). A smooth, well-defined edge to the mass was noted. There were no firm masses within the lesion and no nipple discharge could be elicited. Abdominal, testicular and neurological examination showed no abnormal findings. On assessment of his biochemical endocrinology profile, all parameters were within normal ranges. An ultrasound examination of the left thigh was consistent with mixed density breast tissue but no evidence of malignancy.

Mass inner aspect left thigh.
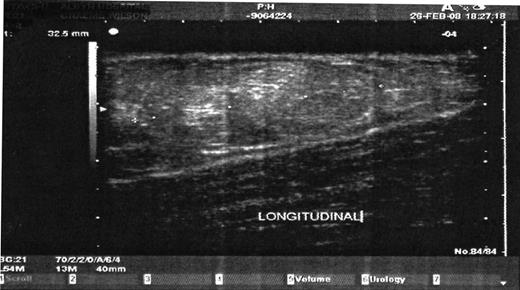
US scan of left thigh lesion.
A mastectomy of this lesion was duly undertaken under general anaesthesia. This was undertaken using simple diathermy. The incision included the nipple areolar complexes and the skin flaps were raised in a manner similar to a standard mastectomy. Complete excision was confirmed by dissection to muscular fascia. Primary closure of the tissues was possible without tension on the superficial tissues.
Histo-pathological analysis of this lesion confirmed the mass to be an ectopic breast mass with no underlying malignancy. This patient had a complete and uneventful recovery. On subsequent review, this gentleman remains well.
DISCUSSION
Breast tissue is modification of sweat glands and is derived from downward migration of ectoderm into the underlying mesenchyme. It develops between the sixth and eight gestational weeks into a thickening of this ectoderm into the embryological milk line [4]. This ridge extends from the axilla to the inguinal region. Humans usually have breasts with associated nipple areolar complexes (which have different embryological development) only in the pectoral region as the rest of the embryological milk line disappears soon after its development. However, if complete degeneration fails to occur, ectopic breasts can develop anywhere along this line [4].
Accessory breasts can develop out-with the milk line, although these lesions are rare. They have been reported previously on the upper aspect of the torso, the neck, the face and the lateral aspect of the thigh [5]. Indeed, Aksoy et al. [5] describe a case of a woman with a similarly placed ectopic breast to our case. Our case differs in that he is male and therefore his underlying ectopic tissues are not subject to the same hormonal influences as a female patient.
Gynaecomastia is enlargement of the ductal and stromal tissue of the male breast and is a common condition amongst peripubertal boys and mature men [1]. This presentation can either be as a result of physiological, iatrogenic (by means of stimulation with medications) or neoplastic processes. It has an incidence of between 30 and 50% in the population [1, 6].
Serpa et al. [6] report ectopic gynaecomastia in a man suffering from long-standing type 1 diabetes. These breasts were found bilaterally in the inguinal region of his abdominal wall. They were identified within the lipohypertrophy associated with his subcutaneous insulin administration [6]. They report the first case of ectopic gynaecomastia in the literature. However, this was only on imaging investigations as no histological assessment was undertaken.
It is of interest that in the case described by Serpa et al., the breast tissue was within the lipohypertrophy of insulin injections. Insulin has known mitogenic properties [7] and the stimulation of this hormone could have assisted in the formation of the breast tissue. No discernable nipple areolar complex was evident in the ectopic breast tissue reported by this group.
The patient in our case had breast tissue discrete from the milk line. This was associated with a nipple areolar complex and the diagnosis was confirmed on histological assessment of the resected tissue. In addition, our case was identified in a man who has no underlying co-morbidities. This has not been reported previously. Preoperative assessment was rigorous both to confirm the diagnosis and to exclude malignancy within the lesion or elsewhere, driving its growth by means of endocrinological factor production.
The inner thigh is a site where breast tissue has been described before in a female case but not in a male patient. In this report, we describe the first histologically proven case of ectopic gynaecomastia in a man with no underlying illnesses.

{kind=link}
{kind=link}
{kind=link}
{kind=link}