





Abstract
We present a rare case of a vesicocutaneous fistula secondary to two large bladder calculi in a patient with spina bifida. A 62 year old lady presented with swelling of her right thigh and a calcified mass protruding through the subcutaneous tissues of her right groin. Urine was seen to be draining from around the area and plain radiographs and a computed topography (CT) scan confirmed the presence of two bladder calculi with a vesicocutaneous fistula. Vesicolithotomy was performed and the fistula tract left to close spontaneously. Worldwide this is only the fourth case of a bladder calculus causing a vesicocutaneous fistula.
INTRODUCTION
Bladder calculi have been a cause of significant morbidity for thousands of years. Although uncommon in the western world they account for 5% of urinary calculi. (1) Patients may report dysuria, intermittency, haematuria, frequency, hesitancy, nocturia or sudden termination of voiding. A rare complication of bladder calculi is that of vesicocutaneous fistula. We report the fourth case worldwide of a vesicocutaneous fistula caused by bladder calculi. (2-4)
CASE REPORT
A 62 year old lady presented to the hospital with a swelling in her right thigh. She had a past history of myelomeningocele spina bifida which had been closed at birth. As a result she had no motor function or sensation in her lower limbs. Sensation was recorded as being absent below the T12 dermatome. She suffered from urinary incontinence and had been managed with long term suprapubic catheters for 20 years. She had required a vesicolithotomy via a midline incision and a vaginal hysterectomy 13 years previously.
Initial examination revealed a swollen right thigh and a calcified mass protruding through the skin in the right groin. A strong smell of urine was noted although it was thought that this was secondary to a leakage from around the site of her supra pubic catheter. Laboratory data demonstrated normal renal function, a raised C-reactive protein and normal white cell count. Due to her swollen right leg a deep vein thrombosis was excluded with an Ultrasound scan and negative D Dimer and plain radiographs of her right hip and pelvis were requested.
A urology opinion was sought, initially, with regard to management of the suprapubic catheter. On closer examination, urine was noted to be leaking not from the suprapubic site but around the calcified mass in the right groin and a diagnosis of vesicocutaneous fistula was made. Her radiographs demonstrated two urinary calculi (Fig 1) and she went on to have an abdominal computed topography scan (Fig 2 ) which confirmed the diagnosis of a vesicocutaneous fistula.
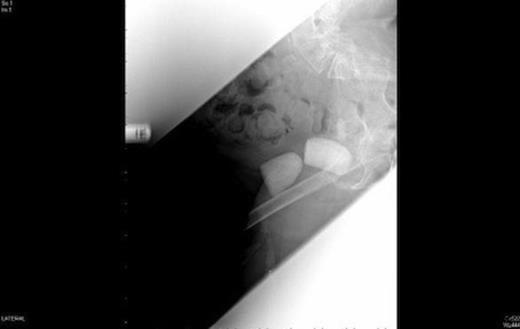
Plain Radiographs demonstrating two bladder calculi
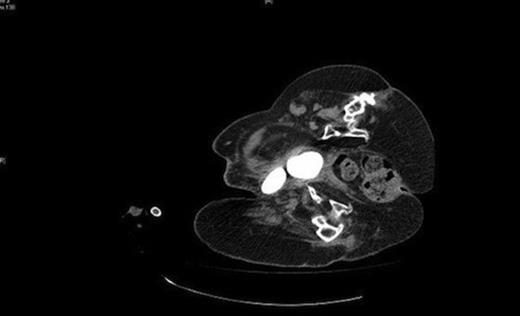
CT demonstrating the two bladder calculi pointing towards the right groin
Vesicolithotomy was performed removing the calculi by enlarging the fistulous opening. (Fig 3) Two calculi measuring 40mm × 43mm × 30mm and 43mm × 50mm × 33mm were extracted. (Fig. 4) The suprapubic catheter was changed and the fistula was left open and urine leakage continued to decrease in quantity until the fistula tract closed.

Intraoperative view of the bladder calculi emerging through the vesicocutaneous fistula into the right groin

The two bladder calculi following extraction
DISCUSSION
The management of urological problems in patients with spina bifida can be very challenging. Urological complications are often a major source of morbidity for these patients. (5) Abnormal bladder sensation and function combined with sphincter dysnergia predispose the spina bifida patient to urinary stasis, recurrent urinary tract infections, stone formation and renal function impairment. (5) Management of the problem can be difficult and may include the use of anti-cholinergics, intermittent self catheterisation (ISC), supra pubic catheterisation or surgical intervention to allow urinary diversion. (6) Increased fluid intake, weekly changes of indwelling catheters if ISC is not possible and regular ultrasonic screening, to pick up stone formation at an early stage, may help reduce the burden of these problems. (7)
Vesicocutaneous fistula secondary to bladder calculi are rare. Only three cases have been previously reported in the literature. (2-4) Predisposing factors to bladder stone formation include urinary stasis, bladder outflow obstruction urinary stasis, recurrent urinary tract infections and foreign bodies within the bladder (1), all of which can be seen in spina bifida patients. In our case the added sensory abnormalities secondary to spina bifida left the bladder calculus undiagnosed until it had formed the vesicocutaneous fistula. Good control of the predisposing factors can dramatically reduce the risk of developing bladder calculi, but especially in cases where this is difficult, a high index of suspicion, regular urological review and timely USS can prevent the development of both the bladder calculus and its complications.

{kind=link}
{kind=link}
{kind=link}
{kind=link}