





Abstract
An 18 year-old-male sustained a gunshot wound to the abdomen which required an uneventful hepatorrhaphy. He later returned with a large right effusion and was diagnosed with a chylothorax. The output was persistent despite conservative measures. Thoracotomy with attempted thoracic duct ligation was unsuccessful at decreasing the output. Re-exploration and ligation of the thoracic duct was required thru an abdominal approach.
INTRODUCTION
Chylothorax is a condition that results when the thoracic duct or its tributaries is disrupted along its course, leading to the accumulation of chyle within the pleural space. The etiology of chylothorax in adults is usually either traumatic or related to malignancy (1). Traumatic causes are most commonly iatrogenic (post-surgical), but also have been reported after blunt or penetrating trauma, and only rarely requires surgical treatment (2,3). We present a case of a high output chylothorax which resulted following a gunshot injury to the abdomen which required an unorthodox surgical approach to correct.
CASE REPORT
An 18 year-old-male patient presented to our trauma center following a gun shot wound to the abdomen. On arrival, he was found to have a penetrating injury to the epigastrium with no apparent exit wound. He was hemodynamically stable and a CXR demonstrated a metallic foreign body in the upper abdomen. On physical exam, he was tender to palpation. The patient was taken to the operating room for an emergency laparotomy. During surgery, a laceration of the liver was identified and repaired with omental packing (Figure 1). A large bullet fragment was palpable within the injured segment of liver and was removed. The patient had an uneventful recovery and was discharged home on post-op day 3.
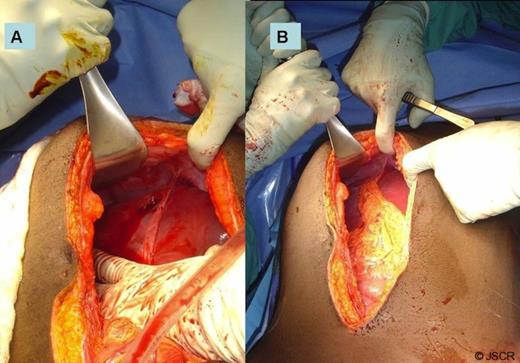
Liver injury with cavitary defect (A). Repair with Omental packing (B).
Six days later, the patient returned to the emergency department with complaints of right sided chest pain and worsening dyspnea. A plain chest film was performed (Figure 2) and demonstrated a large right pleural effusion. Computerized tomography of the abdomen also demonstrated several tiny retained metallic fragments embedded within the liver and retroperitoneum (Figure 3). A chest tube was inserted on the right side and immediately drained 2.2L of milky fluid (Figure 4).

eturn CXR with large right effusion.

Computerized tomography of the abdomen demonstrating tiny metallic fragments within liver. Fragment adjacent to aorta suspected of injuring retroperitoneal thoracic duct (arrow).
Chest tube with classic appearance of milky white chyle.
The diagnosis of chylothorax was confirmed after analysis of the fluid revealed elevated triglycerides and the presence of chylomicrons. The patient was initially treated with nothing via the oral route, parenteral nutrition and intravenous somatostatin analog. Despite these conservative measures, the chest tube continued to drain approximately 2-4 liters daily. Having failed conservative therapy, the patient was taken to the operating room for a right-sided thoracotomy and attempted ligation of the thoracic duct. Following this operation, however, there was no improvement in the chest tube output.
A few days later, the interventional radiologists attempted lymphangiography and embolization of the leaking duct (Figure 5). This also proved unsuccessful and did not improve the output. The patient was subsequently taken to the operating room for a re-exploration and attempted ligation of the lymphatic leak transabdominally. During surgery, the right crus was divided and the retroperitoneal tissues to the right of the supraceliac aorta were ligated in an attempt to obstruct the lymphatics draining proximal to the transhepatic injury. Following this operation, there was an immediate decrease in the output from the chest tube associated with an improved chest x-ray. The chest tube was removed on post-op day #7 once the patient tolerated a regular diet without any increase or change in output. The patient was discharged home the next day and has since recovered well from his injury.

Lymphangiogram mapping through groin (A) with attempted embolization of thoracic duct utilizing fluoroscopy (B).
DISCUSSION
Chylothorax is an uncommon complication following trauma. Chylothorax has been reported with thoracic injuries but not previously reported with gunshot injuries to the abdomen. When diagnosed in a delayed fashion, chylothorax is typically managed conservatively with dietary restriction of fats, parenteral nutrition and chest tube drainage. Somatostatin analog and embolization of injured lymphatic ducts has also been described with mixed results. Thoracic duct ligation via a right thoracotomy is indicated for persistent drainage if conservative therapy fails to decrease the output. This approach is only successful if ligation occurs below the area of injury. In our case, we believe that a small metallic fragment injured the intrabdominal retroperitoneal portion of the cisterna chyli or thoracic duct, resulting in a persistent chylothorax despite attempted transthoracic ligation of the duct. Continued output from the chest tube after thoracotomy could be explained by either failure to correctly identify and control the thoracic duct surgically, or an injury that was low enough to continue leaking chyle despite a more distally obstructed duct. We believe the later was the case since the output finally improved once we controlled the thoracic duct and lymphatics below the transhepatic injury. Although less commonly used, the transabdominal approach has been previously described and thought to be advantageous due the thoracic ducts' more consistent proximal anatomical location (4). In summary, chylothorax is a rare complication following abdominal or retroperitoneal trauma and we believe that treatment may require an unorthodox approach, especially with suspected injuries below the thoracic cavity.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}